Cardiovascular Diseases
Cardiovascular diseases cover all diseases of the heart and blood vessels – including heart attacks and strokes, atherosclerosis, ischemic heart disease, hypertensive diseases, cardiomyopathy, and others.
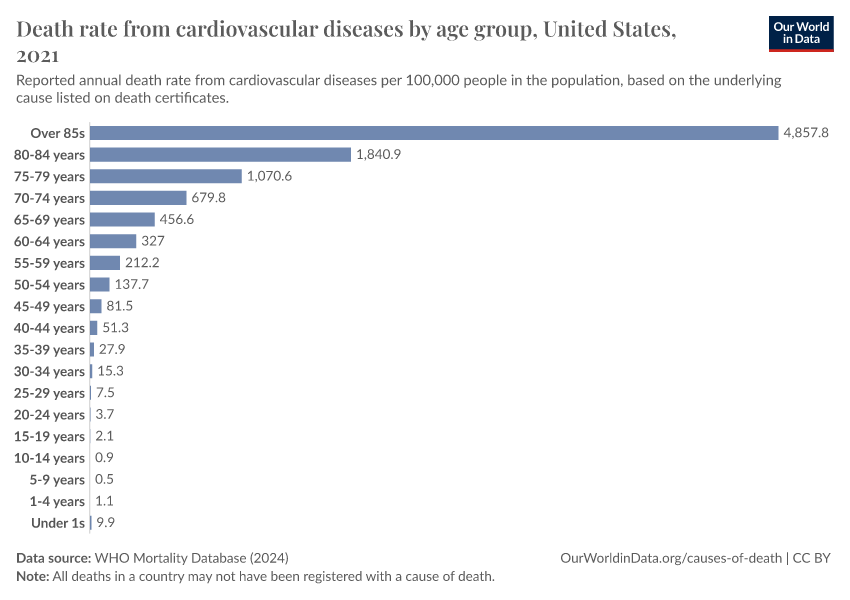
These diseases tend to develop gradually with age, especially when people have risk factors like high blood pressure, smoking, alcohol use, poor diet, and air pollution.
Together, cardiovascular diseases are the most common cause of death globally.
In 2000, around 14 million people died from cardiovascular diseases globally, while in 2019, close to 18 million died.
The rising death toll is largely due to a growing and aging global population. Death rates from cardiovascular diseases have actually fallen in many countries – as our ability to prevent and treat them has improved.
Large declines in smoking; improvements in screening, diagnosis, and monitoring; and advances in medical treatments, public health initiatives, emergency care, and surgical procedures, have all helped to reduce the impact of cardiovascular diseases on people’s lives.
Yet large disparities remain globally. The impact of cardiovascular diseases can be reduced much further with greater understanding and public health efforts.
On this page, you will find global data on cardiovascular diseases, their risk factors and treatments, and their trends over time.
Key Insights on Cardiovascular Diseases
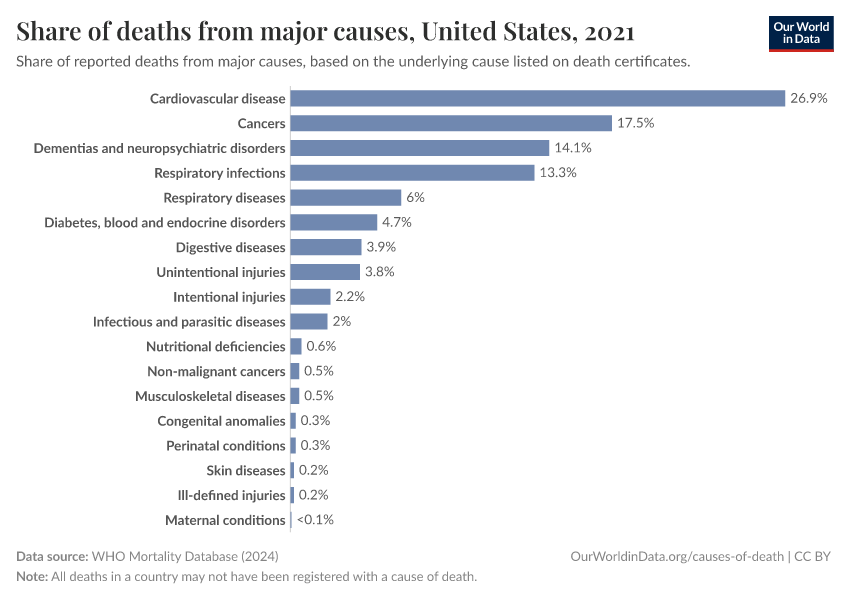
Cardiovascular diseases are the most common cause of death worldwide
This chart shows what people died from globally in 2019. Each box represents a cause of death, and the size of each box is proportional to the number of deaths it caused.
As you can see, heart diseases and other cardiovascular diseases are the most common causes of death, responsible for a third of all deaths globally, a total of around 18 million.
Cardiovascular diseases are part of a larger group of diseases called non-communicable diseases, which are shown in blue in the visualization. These are diseases that tend to develop gradually over time and can’t be passed on to other people,1 and also includes cancers, chronic respiratory diseases, and other chronic diseases.
Taken together, these non-communicable diseases are the cause of around three-quarters of all deaths globally.
In this article, we cover this in more detail:
What you should know about this data
- This data comes from the 2019 publication of the Global Burden of Disease study by the Institute for Health Metrics and Evaluation (IHME). The one exception is the data on deaths from terrorism, which comes from the Global Terrorism Database.
- These estimates assign each death a single cause based on data on the underlying cause of death listed on death certificates, verbal autopsies, and statistical modeling. This is a simplification, as people often have multiple diseases or injuries that contribute to their death, which may also be listed on death certificates.
- This chart shows data on causes of death globally for 2019, the year before the COVID-19 pandemic started.
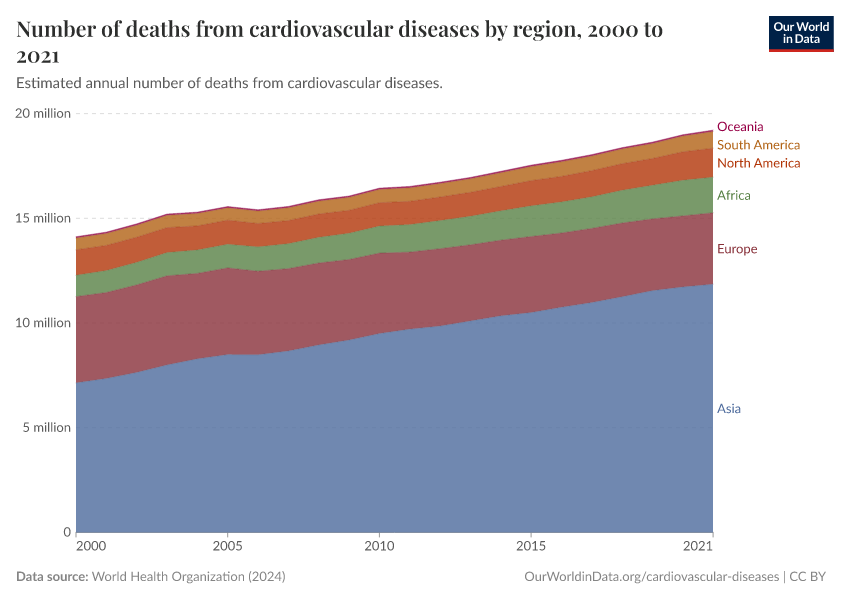
The global death toll from cardiovascular diseases has grown
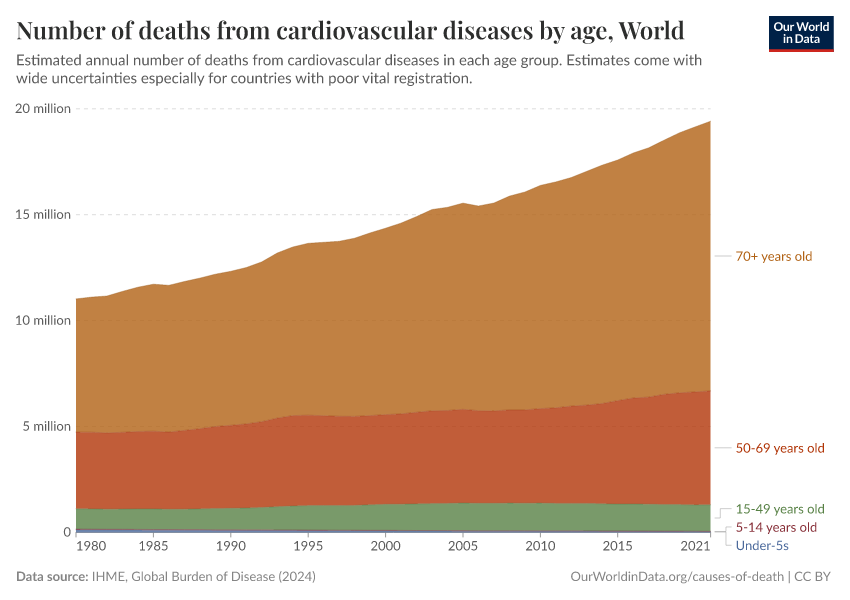
The total number of deaths from cardiovascular diseases has risen globally.
In 2000, around 14 million people died from cardiovascular diseases globally, while in 2019, that figure was almost 18 million.
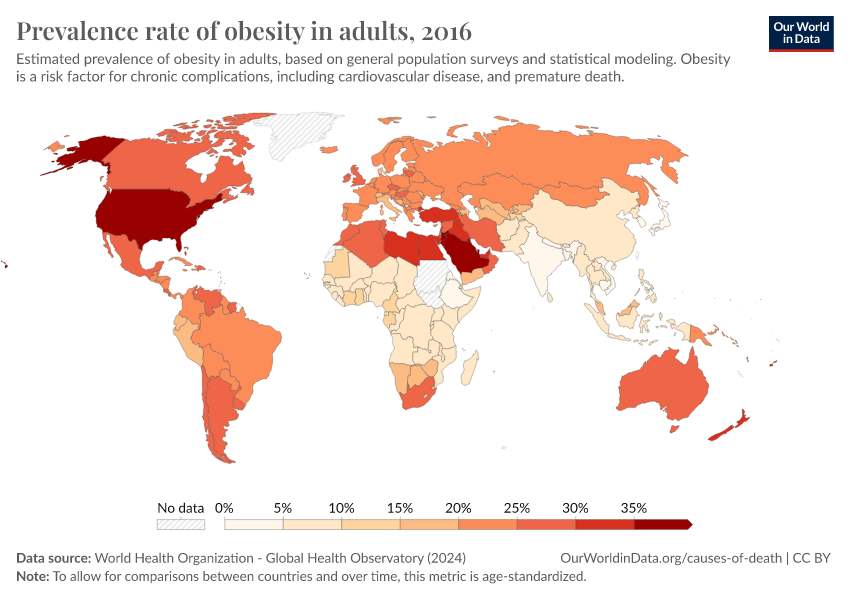
This rise is partly due to a growing and aging population, especially in Asia, as well as increases in risk factors such as obesity and diabetes.2
As some of these trends will continue in the coming decades – particularly with the increasing number of elderly people across the world – cardiovascular diseases are likely to become a larger burden on healthcare systems.
What you should know about this data
- These estimates assign each death a single cause based on data on the underlying cause of death listed on death certificates, verbal autopsies, and statistical modeling. This is a simplification, as people often have multiple diseases or injuries that contribute to their death, which may also be listed on death certificates.

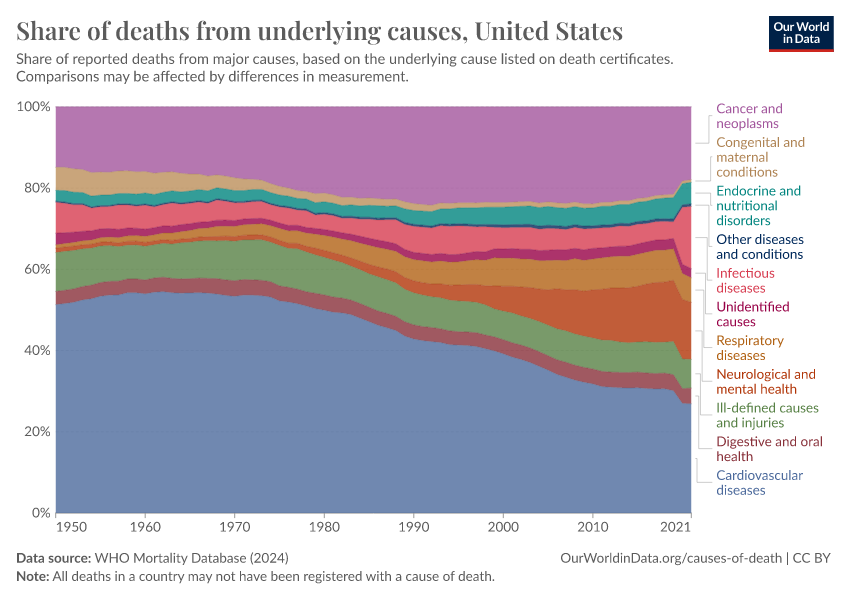
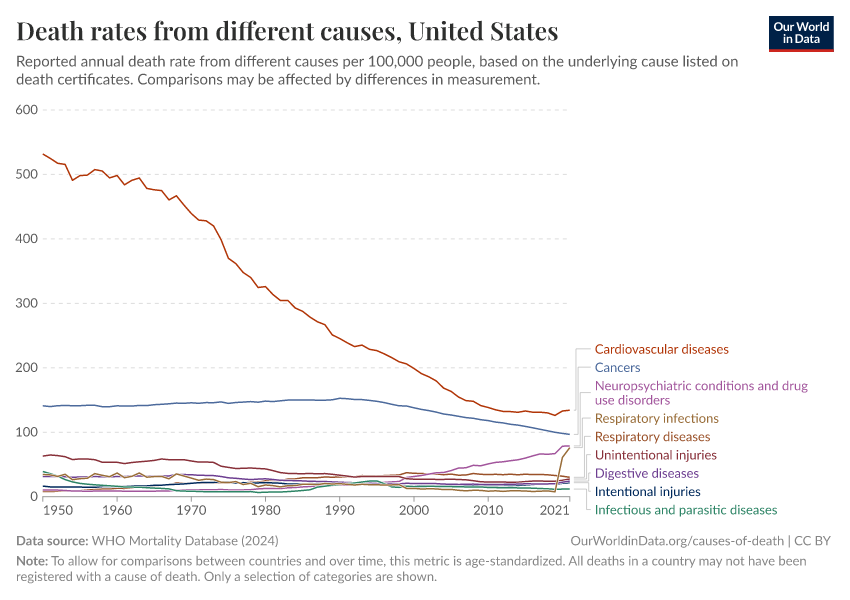
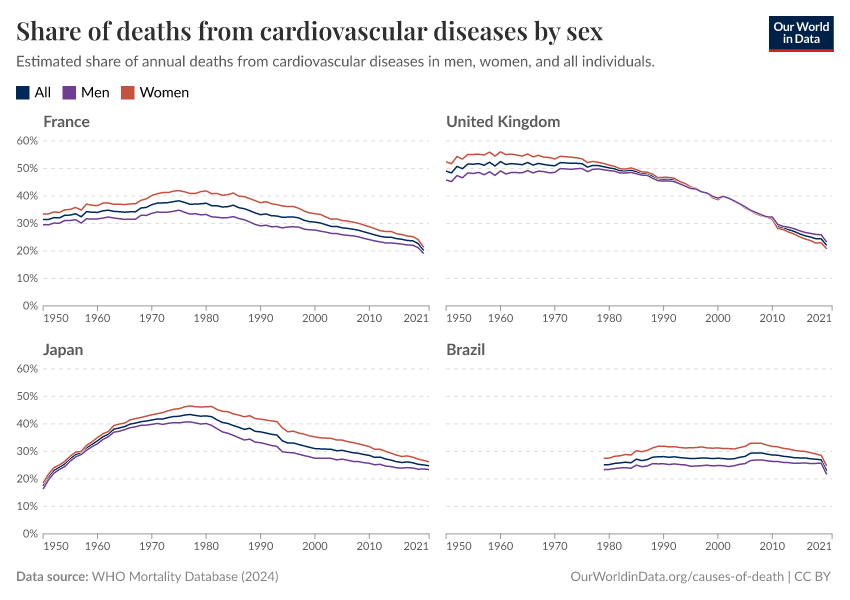
Death rates from cardiovascular diseases have declined in many countries
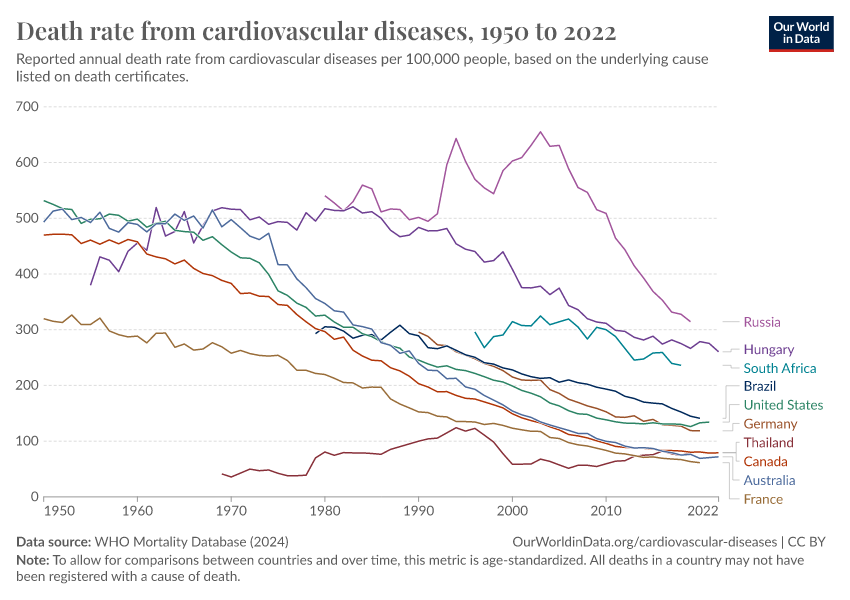
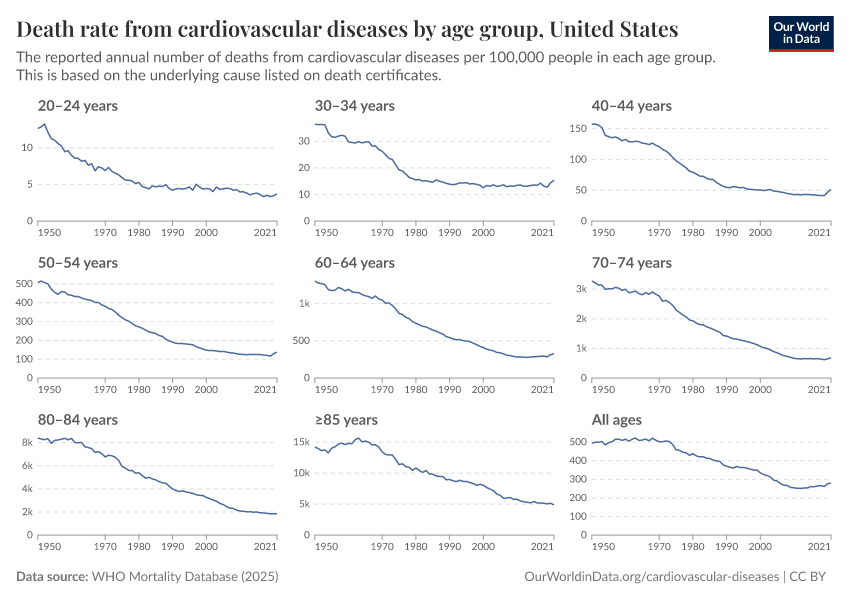
The number of deaths from cardiovascular diseases is increasing, but — as this chart shows — the death rate has declined in many countries.
This means that the risk of death from cardiovascular diseases now is lower than in the past among populations of the same size and age.
In many countries, the decline in death rates has been large, as you can see in the chart.
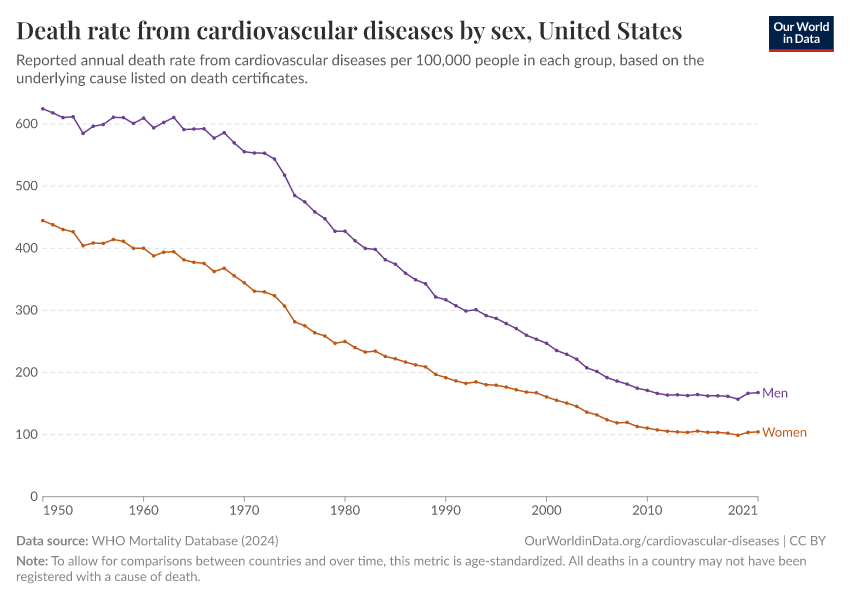
In the United States, for example, the age-standardized death rate from cardiovascular diseases was over 500 per 100,000 people in 1950 and declined to less than 150 in 2020. This represents a reduction of almost three-quarters.
The dramatic decline in smoking has played a significant role in this reduction.3 But during the 20th and 21st centuries, we have also achieved major advances in screening, diagnosis and monitoring, and developed public health initiatives, emergency care, medical treatment, devices, and surgeries, that have helped reduce the consequences of cardiovascular diseases.4
What you should know about this data
- This data comes from the World Health Organization (WHO)’s Mortality Database, which compiles deaths reported by each country annually, based on the underlying cause of death listed on death certificates.
- Countries are only included in the WHO Mortality Database if at least 65% of the deaths that occurred in a given year were registered in vital registration systems and reported to the WHO.
- The data has been age-standardized, which allows for comparisons between different countries and over time, where populations have different age structures. However, declines are also seen when using crude death rates. You can read more about crude and age-standardized rates in our article on age standardization.

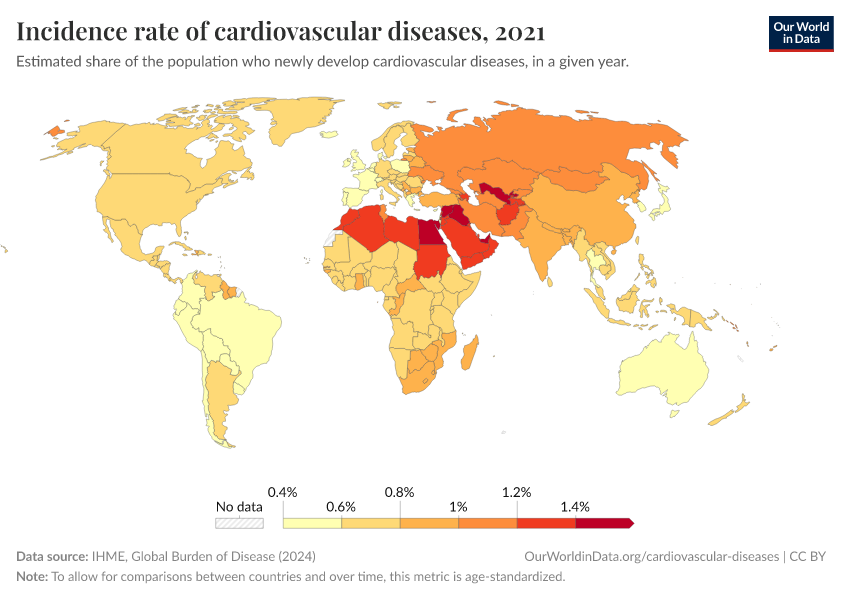
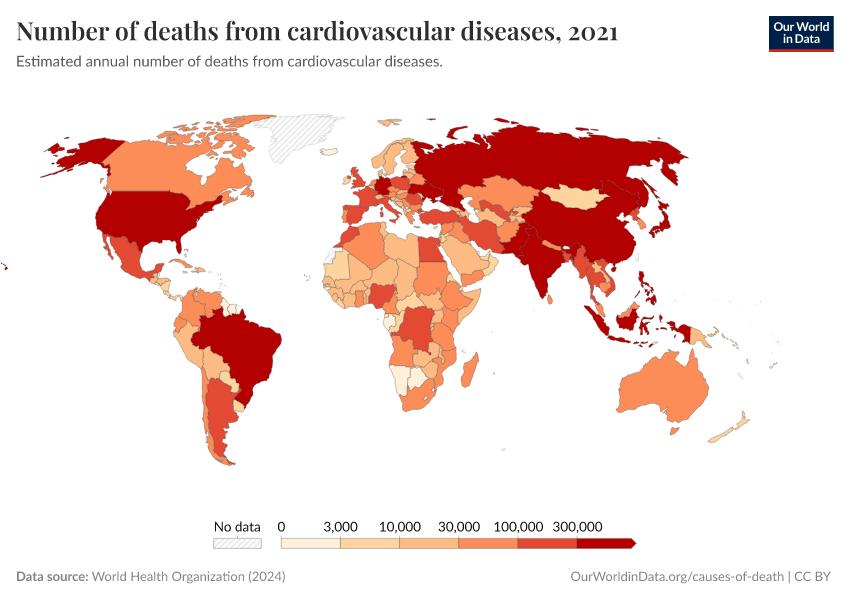
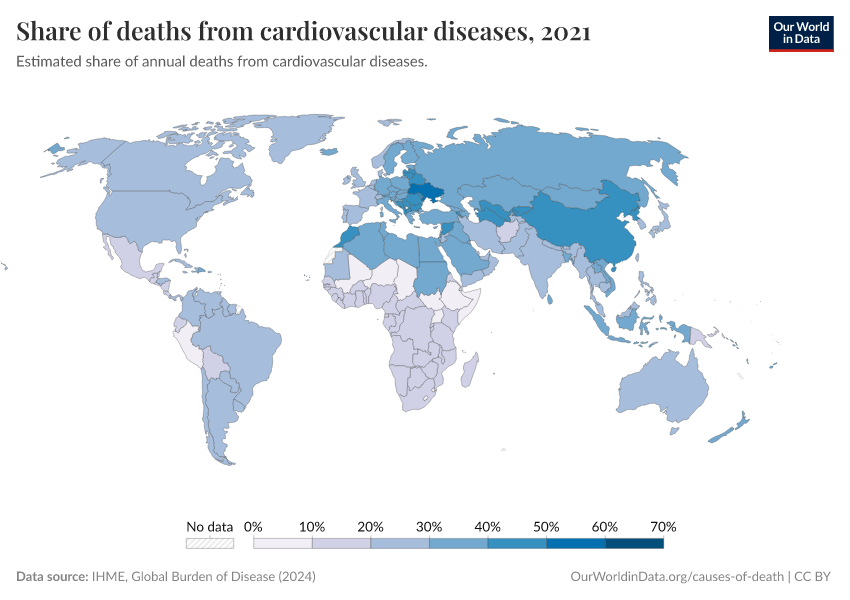
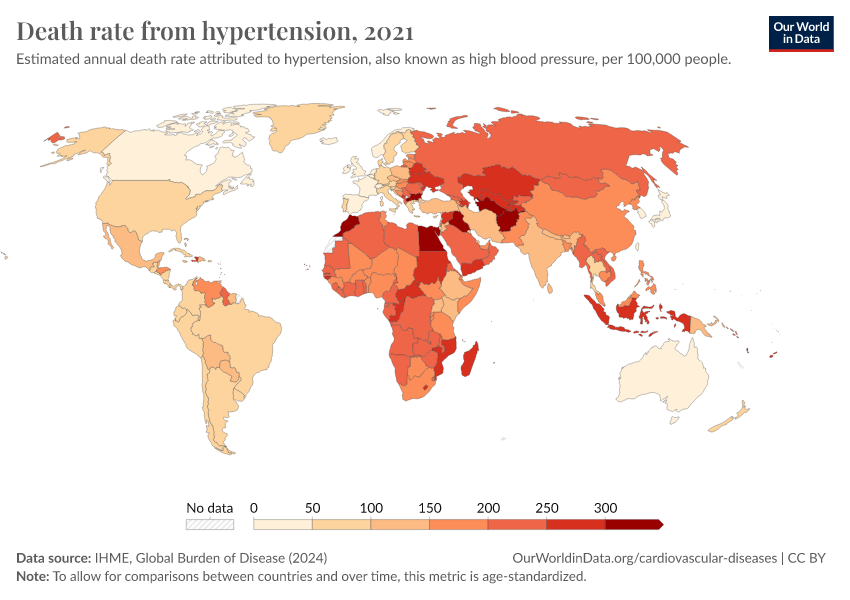
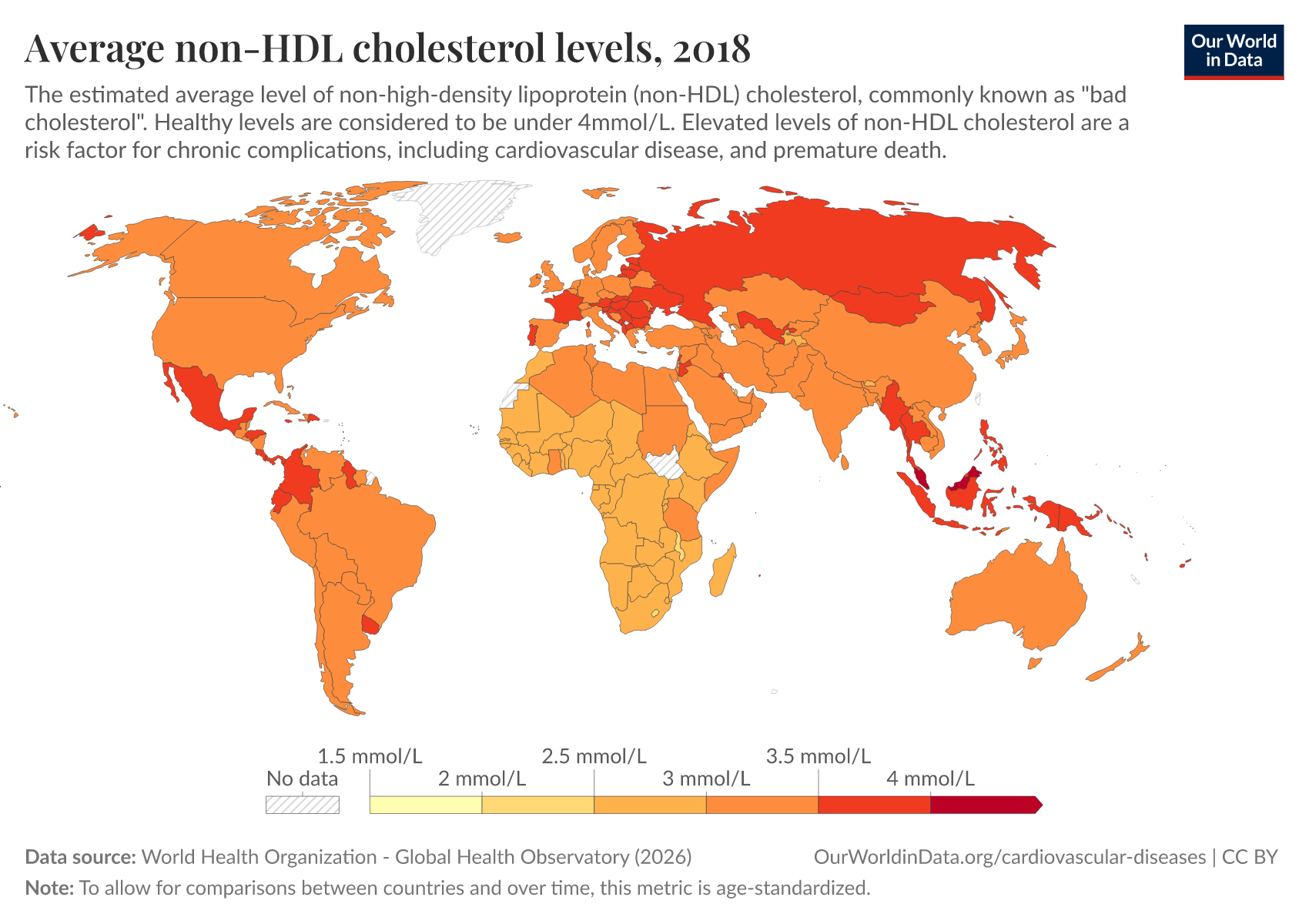
There are large disparities in death rates from cardiovascular diseases worldwide
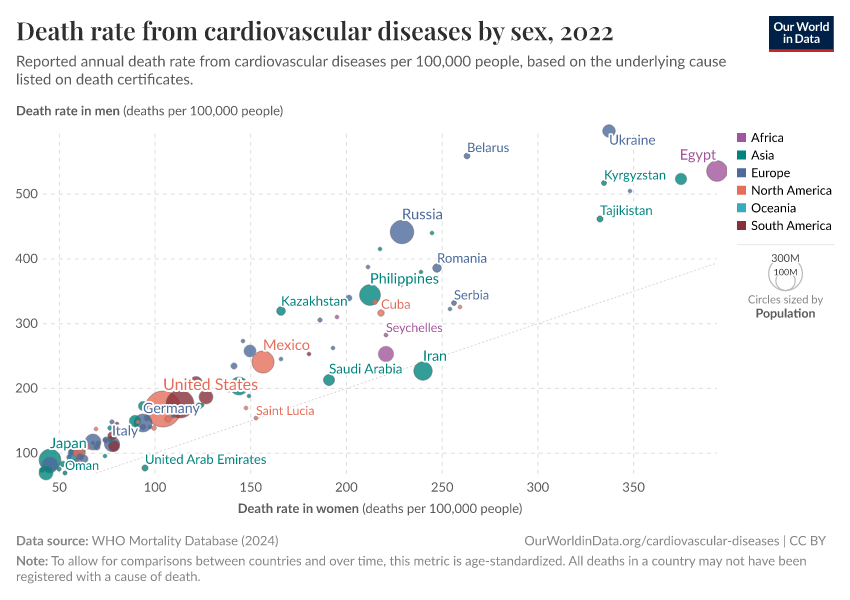
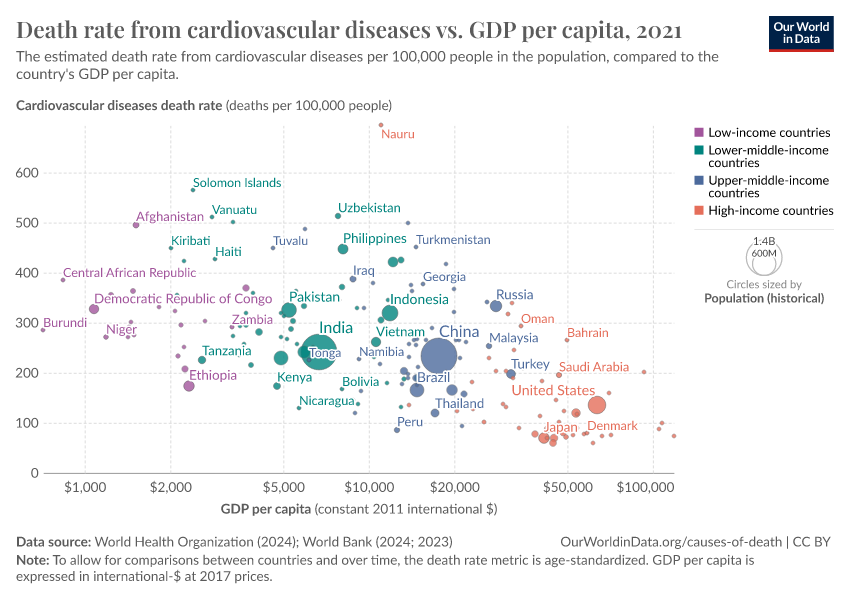
Death rates from cardiovascular diseases vary widely between countries.
As shown in the map, they tend to be higher in Africa, Asia, Eastern Europe, and South America than in North America and Western Europe.
In France, Australia, and Canada, the estimated death rate was less than 80 per 100,000 people in 2019. While in Afghanistan, Sudan, and Mongolia, it was more than 500.
These wide differences arise from differences in risk factors – such as smoking, alcohol consumption, and air pollution – as well as lower healthcare access and investment to screen and treat cardiovascular diseases, which can require long-term management.2
What you should know about this data
- This data comes from the World Health Organization’s Global Health Estimates.
- These estimates assign each death a single cause based on data on the underlying cause of death listed on death certificates, verbal autopsies, and statistical modeling. This is a simplification, as people often have multiple diseases or injuries that contribute to their death, which may also be listed on death certificates.

A range of factors heighten the risk of cardiovascular diseases
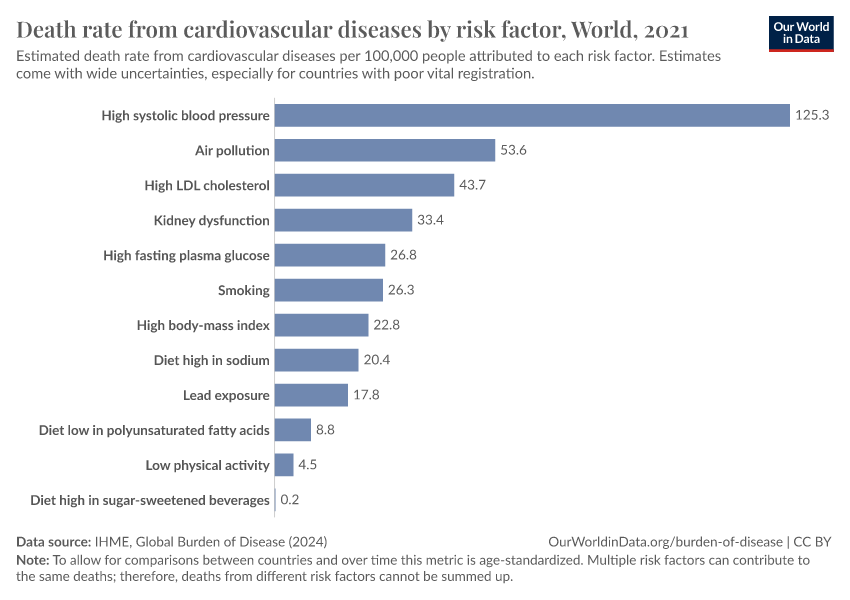
Different types of risk factors increase the risk of cardiovascular diseases.
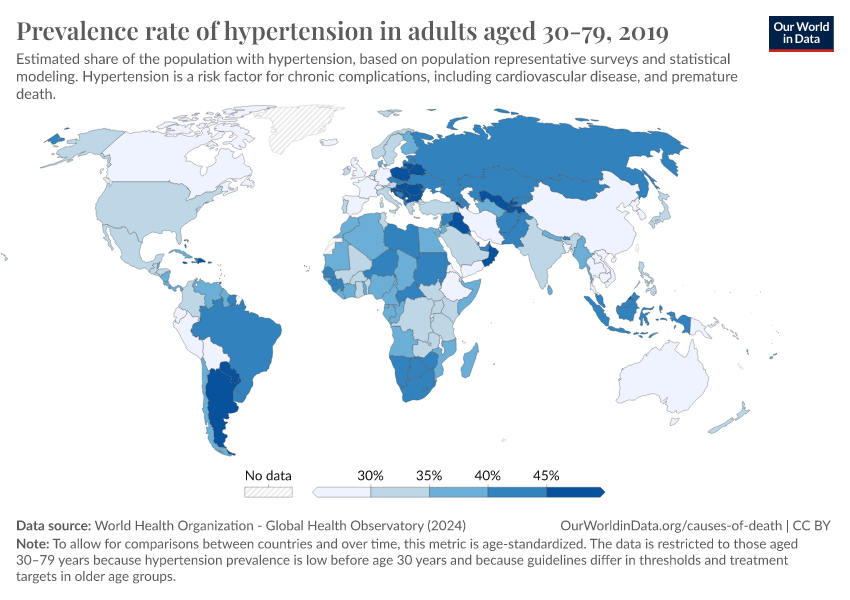
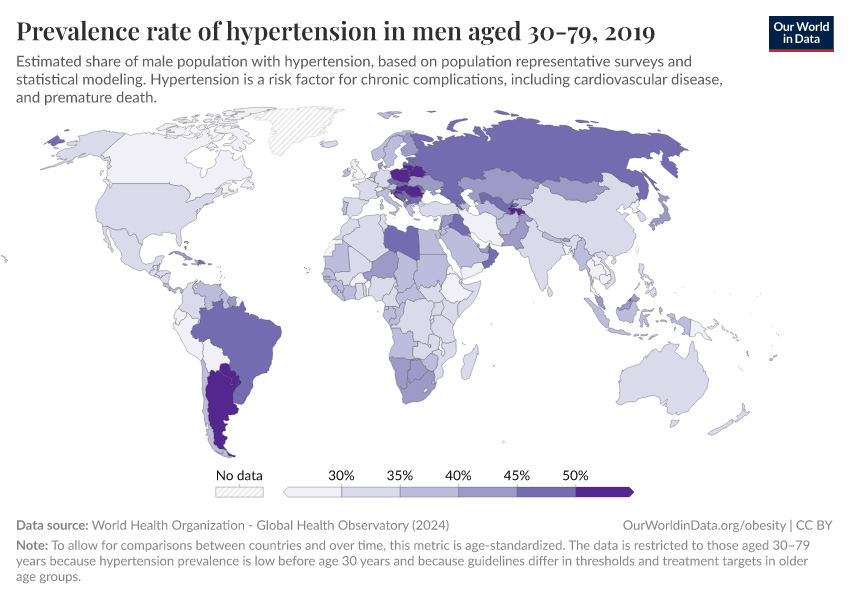
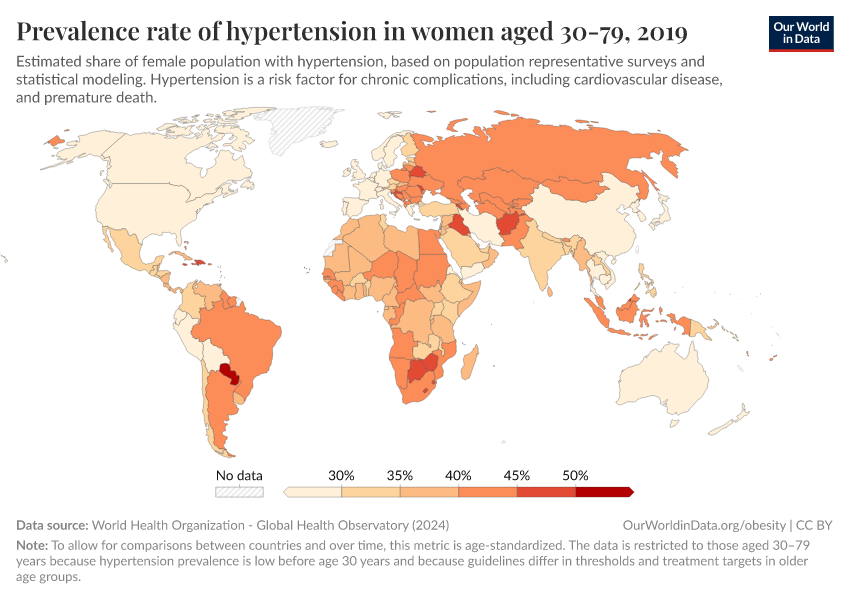
This includes behaviors such as smoking, alcohol use, and diets high in sugar and sodium; clinical risk factors, such as high blood pressure and high LDL cholesterol; and environmental risks, such as air pollution and lead exposure.5
The chart shows the estimated number of deaths from cardiovascular diseases attributed to each risk factor.
High blood pressure, or hypertension, is the number one risk factor. It’s estimated that it causes almost 10 million deaths from cardiovascular diseases annually.6
What you should know about this data
- These estimates come from the Global Burden of Disease study by the Institute for Health Metrics and Evaluation (IHME).
- Although precise numbers are shown, these estimates have uncertainties. These arise partly from uncertainties in the number of deaths from cardiovascular diseases, and from uncertainties in the prevalence and impact of risk factors. This is especially true in poorer countries where death registration and surveys may be lacking.
- The researchers estimate the number of deaths caused by each risk factor in several steps. First, they estimate the increased mortality risk caused by each risk factor. This is measured relative to a theoretical minimum (for example, the absence of the risk factor or its reduction to an optimum level). Next, they estimate the number of people exposed to the risk factor. Finally, they combine these to estimate the number of deaths caused by the risk factor.
- The impacts of risk factors are not exclusive: people can be exposed to multiple risk factors, and some are related and can interact. Therefore, the numbers shown here do not sum up to the total deaths from cardiovascular diseases.

Research & Writing
August 4, 2025
Death rates from cardiovascular disease have fallen dramatically — what were the breakthroughs behind this?
Over a century of progress in surgery, drugs, prevention, and emergency response has driven down death rates from heart disease and stroke.
December 14, 2023
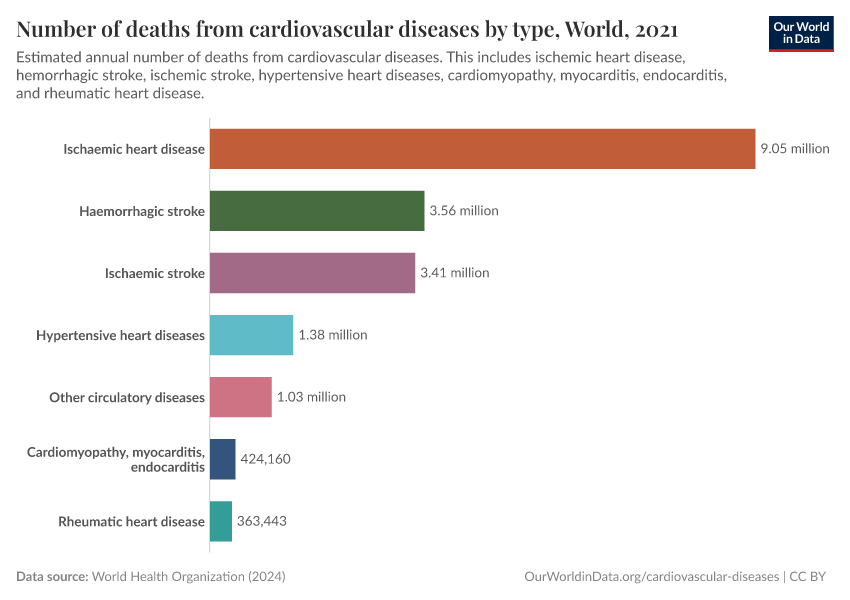
What are the different types of cardiovascular diseases, and how many deaths do they cause?
Cardiovascular diseases are a range of related health conditions that develop in the heart and blood vessels. What are the different diseases, and what is their impact worldwide?
More articles on cardiovascular diseases and their risk factors
Key Charts on Cardiovascular Diseases
See all charts on this topic

























































Featured Data on Cardiovascular Diseases
Endnotes
Although communicable and non-communicable diseases are shown separately, it is now understood that infectious diseases contribute to several non-communicable diseases.
This includes Helicobacter pylori and stomach cancer, human papillomavirus and cervical cancer, hepatitis C virus, and liver cancer, Chlamydia pneumoniae and atherosclerosis, Streptococcus pneumoniae and chronic respiratory diseases, and others.
In addition, infectious diseases can increase the risk of dying from non-communicable diseases. For example, several respiratory pathogens, such as the influenza virus, increase the risk of heart attacks and strokes.
Mercer, A. J. (2018). Updating the epidemiological transition model. Epidemiology and Infection, 146(6), 680–687. https://doi.org/10.1017/S0950268818000572
Behrouzi, B., Bhatt, D. L., Cannon, C. P., Vardeny, O., Lee, D. S., Solomon, S. D., & Udell, J. A. (2022). Association of Influenza Vaccination With Cardiovascular Risk: A Meta-analysis. JAMA Network Open, 5(4), e228873. https://doi.org/10.1001/jamanetworkopen.2022.8873
Jagannathan, R., Patel, S. A., Ali, M. K., & Narayan, K. M. V. (2019). Global Updates on Cardiovascular Disease Mortality Trends and Attribution of Traditional Risk Factors. Current Diabetes Reports, 19(7), 44. https://doi.org/10.1007/s11892-019-1161-2
Joseph, P., Leong, D., McKee, M., Anand, S. S., Schwalm, J.-D., Teo, K., Mente, A., & Yusuf, S. (2017). Reducing the Global Burden of Cardiovascular Disease, Part 1: The Epidemiology and Risk Factors. Circulation Research, 121(6), 677–694. https://doi.org/10.1161/CIRCRESAHA.117.308903
Roth, G. A., Forouzanfar, M. H., Moran, A. E., Barber, R., Nguyen, G., Feigin, V. L., Naghavi, M., Mensah, G. A., & Murray, C. J. L. (2015). Demographic and Epidemiologic Drivers of Global Cardiovascular Mortality. New England Journal of Medicine, 372(14), 1333–1341. https://doi.org/10.1056/NEJMoa1406656
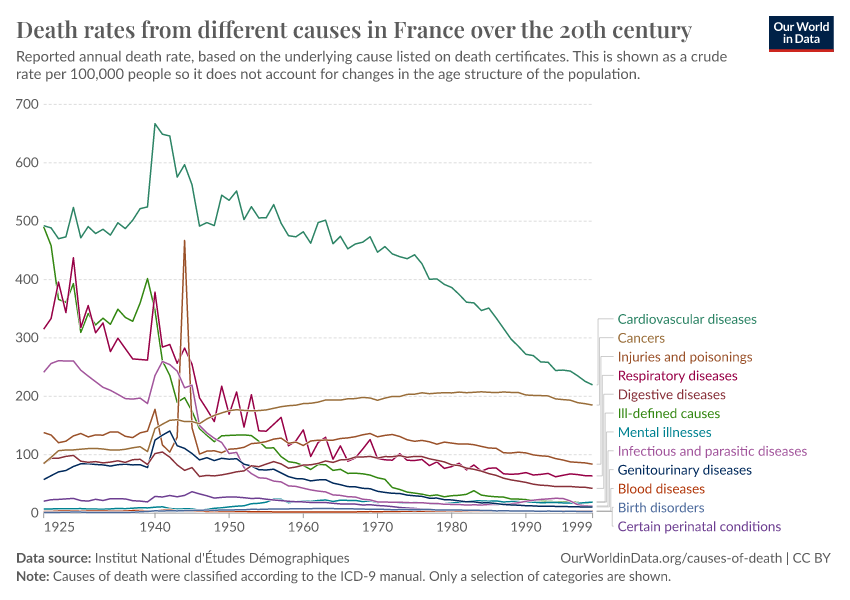
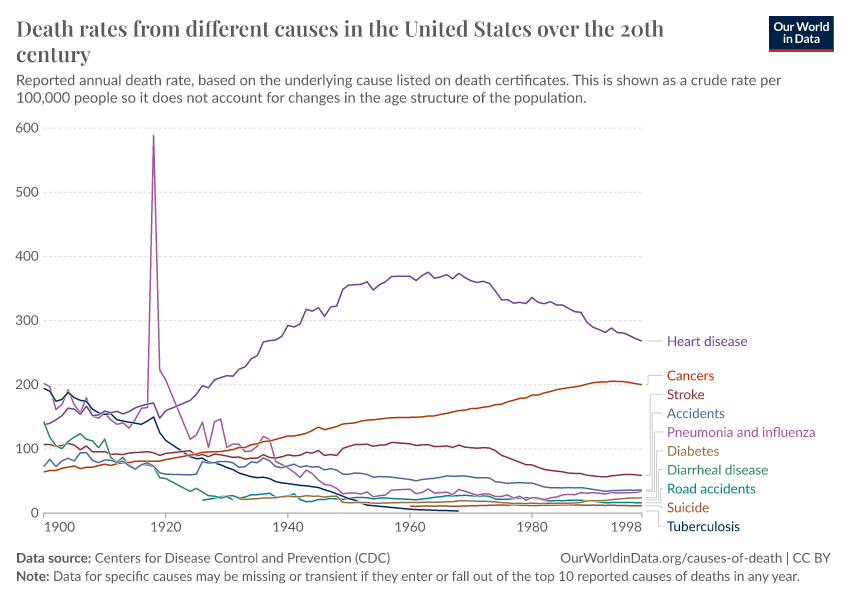
In these related charts, you can see trends in crude death rates from different causes over the twentieth century in France and the United States.
The decline in smoking has a much quicker effect in alleviating the risks of cardiovascular diseases than of lung cancers and other cancers.
Oza, S., Thun, M. J., Henley, S. J., Lopez, A. D., & Ezzati, M. (2011). How many deaths are attributable to smoking in the United States? Comparison of methods for estimating smoking-attributable mortality when smoking prevalence changes. Preventive Medicine, 52(6), 428–433. https://doi.org/10.1016/j.ypmed.2011.04.007
Mensah, G. A., Wei, G. S., Sorlie, P. D., Fine, L. J., Rosenberg, Y., Kaufmann, P. G., Mussolino, M. E., Hsu, L. L., Addou, E., Engelgau, M. M., & Gordon, D. (2017). Decline in Cardiovascular Mortality: Possible Causes and Implications. Circulation Research, 120(2), 366–380. https://doi.org/10.1161/CIRCRESAHA.116.309115
Weisfeldt, M. L., & Zieman, S. J. (2007). Advances In The Prevention And Treatment Of Cardiovascular Disease. Health Affairs, 26(1), 25–37. https://doi.org/10.1377/hlthaff.26.1.25
Gao, Y., Shah, L. M., Ding, J., & Martin, S. S. (2023). US Trends in Cholesterol Screening, Lipid Levels, and Lipid‐Lowering Medication Use in US Adults, 1999 to 2018. Journal of the American Heart Association, 12(3), e028205. https://doi.org/10.1161/JAHA.122.028205
Jagannathan, R., Patel, S. A., Ali, M. K., & Narayan, K. M. V. (2019). Global Updates on Cardiovascular Disease Mortality Trends and Attribution of Traditional Risk Factors. Current Diabetes Reports, 19(7), 44. https://doi.org/10.1007/s11892-019-1161-2
Joseph, P., Leong, D., McKee, M., Anand, S. S., Schwalm, J.-D., Teo, K., Mente, A., & Yusuf, S. (2017). Reducing the Global Burden of Cardiovascular Disease, Part 1: The Epidemiology and Risk Factors. Circulation Research, 121(6), 677–694. https://doi.org/10.1161/CIRCRESAHA.117.308903
Roth, G. A., Forouzanfar, M. H., Moran, A. E., Barber, R., Nguyen, G., Feigin, V. L., Naghavi, M., Mensah, G. A., & Murray, C. J. L. (2015). Demographic and Epidemiologic Drivers of Global Cardiovascular Mortality. New England Journal of Medicine, 372(14), 1333–1341. https://doi.org/10.1056/NEJMoa1406656
Bittner, V. (2020). The New 2019 AHA/ACC Guideline on the Primary Prevention of Cardiovascular Disease. Circulation, 142(25), 2402–2404. https://doi.org/10.1161/CIRCULATIONAHA.119.040625
Jagannathan, R., Patel, S. A., Ali, M. K., & Narayan, K. M. V. (2019). Global Updates on Cardiovascular Disease Mortality Trends and Attribution of Traditional Risk Factors. Current Diabetes Reports, 19(7), 44. https://doi.org/10.1007/s11892-019-1161-2
Kaptoge, S., Pennells, L., De Bacquer, D., Cooney, M. T., Kavousi, M., Stevens, G., Riley, L. M., Savin, S., Khan, T., Altay, S., Amouyel, P., Assmann, G., Bell, S., Ben-Shlomo, Y., Berkman, L., Beulens, J. W., Björkelund, C., Blaha, M., Blazer, D. G., … Di Angelantonio, E. (2019). World Health Organization cardiovascular disease risk charts: Revised models to estimate risk in 21 global regions. The Lancet Global Health, 7(10), e1332–e1345. https://doi.org/10.1016/S2214-109X(19)30318-3
Cosselman, K. E., Navas-Acien, A., & Kaufman, J. D. (2015). Environmental factors in cardiovascular disease. Nature Reviews Cardiology, 12(11), 627–642. https://doi.org/10.1038/nrcardio.2015.152
Newby, D. E., Mannucci, P. M., Tell, G. S., Baccarelli, A. A., Brook, R. D., Donaldson, K., Forastiere, F., Franchini, M., Franco, O. H., Graham, I., Hoek, G., Hoffmann, B., Hoylaerts, M. F., Künzli, N., Mills, N., Pekkanen, J., Peters, A., Piepoli, M. F., Rajagopalan, S., & Storey, R. F. (2015). Expert position paper on air pollution and cardiovascular disease. European Heart Journal, 36(2), 83–93. https://doi.org/10.1093/eurheartj/ehu458
This death toll is a population-attributable number, which means it is an estimate of the number of deaths that would be prevented if hypertension was absent in the entire population.
Cite this work
Our articles and data visualizations rely on work from many different people and organizations. When citing this topic page, please also cite the underlying data sources. This topic page can be cited as:
Saloni Dattani, Veronika Samborska, Hannah Ritchie, and Max Roser (2023) - “Cardiovascular Diseases” Published online at OurWorldinData.org. Retrieved from: 'https://ourworldindata.org/cardiovascular-diseases' [Online Resource]BibTeX citation
@article{owid-cardiovascular-diseases,
author = {Saloni Dattani and Veronika Samborska and Hannah Ritchie and Max Roser},
title = {Cardiovascular Diseases},
journal = {Our World in Data},
year = {2023},
note = {https://ourworldindata.org/cardiovascular-diseases}
}Reuse this work freely
All visualizations, data, and articles produced by Our World in Data are completely open access under the Creative Commons BY license. You have the permission to use, distribute, and reproduce these in any medium, provided the source and authors are credited.
The data produced by third parties and made available by Our World in Data is subject to the license terms from the original third-party authors. We will always indicate the original source of the data in our documentation, so you should always check the license of any such third-party data before use and redistribution.
All of our charts can be embedded in any site.