Tuberculosis
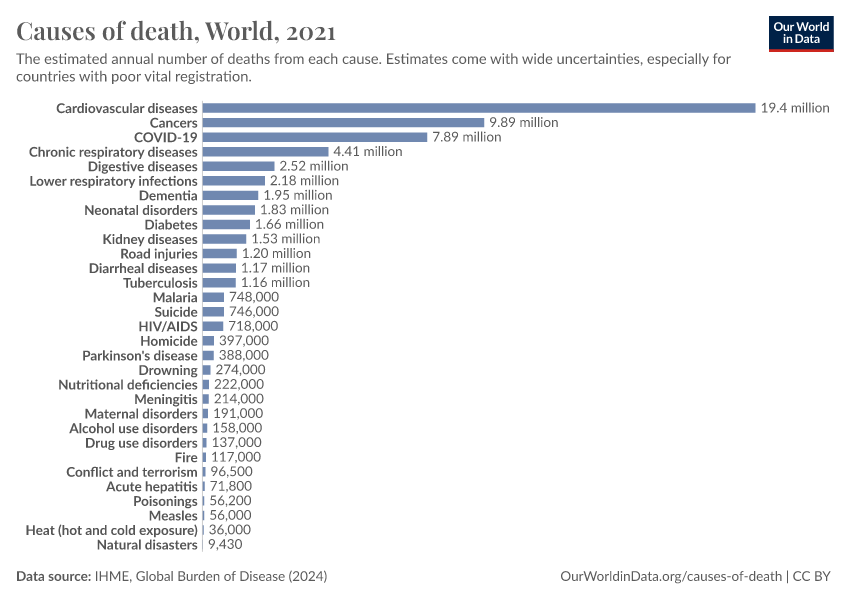
Tuberculosis is one of the most common causes of death globally.
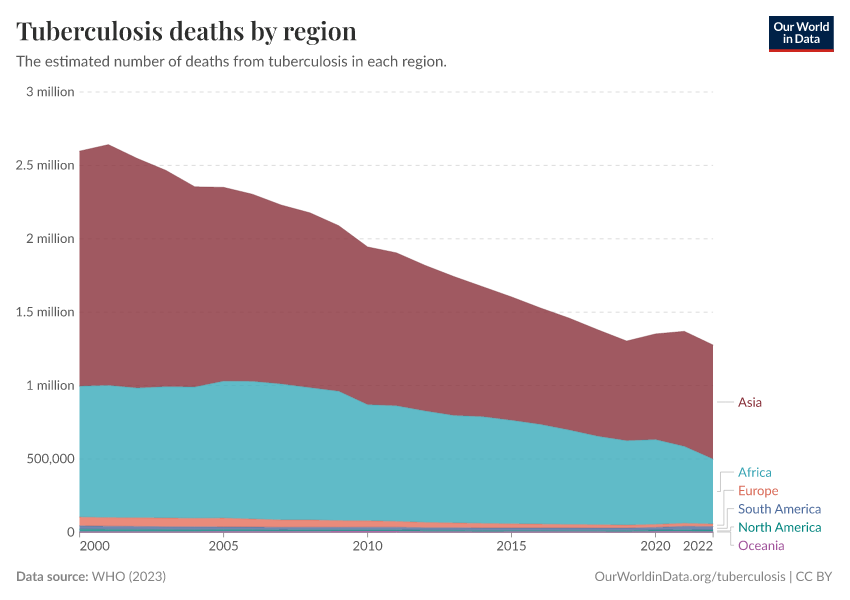
In richer countries, the impact of tuberculosis has been reduced significantly over history, but in poorer parts of our world, it continues to be a major challenge even today: it causes an estimated 1.2 million deaths annually.
Tuberculosis is caused by the bacteria Mycobacterium tuberculosis.
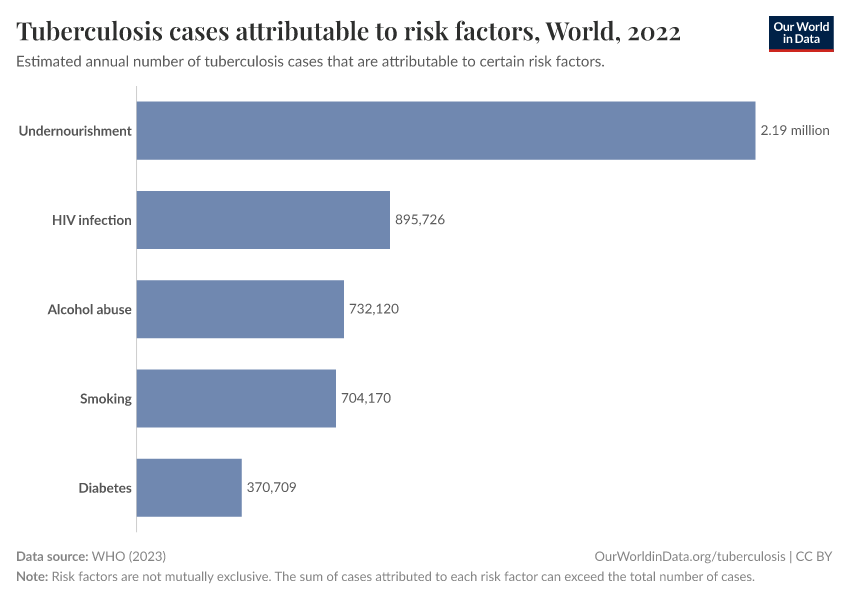
The bacteria spreads through respiratory particles and tends to cause tuberculosis in people with risk factors such as undernourishment, HIV/AIDS, smoking, and existing chronic conditions.
The disease involves symptoms like coughing, fatigue and night sweats, and can damage the lungs, the brain, kidneys and other organs, which can be fatal.
But it is treatable with a combination of specific antibiotics. Without being diagnosed correctly, however, people do not receive the proper treatment. This leaves them vulnerable, and also increases the risk that antibiotic-resistant strains of the bacteria will develop, which are much more difficult and expensive to treat.
With greater effort to tackle its risk factors and improve testing and treatment for the disease, the world can relegate tuberculosis to history — not just in the richer parts of the world, but for everyone.
On this page, you will find global data and trends on tuberculosis, including testing, treatment, and vaccination.
Key Insights on Tuberculosis
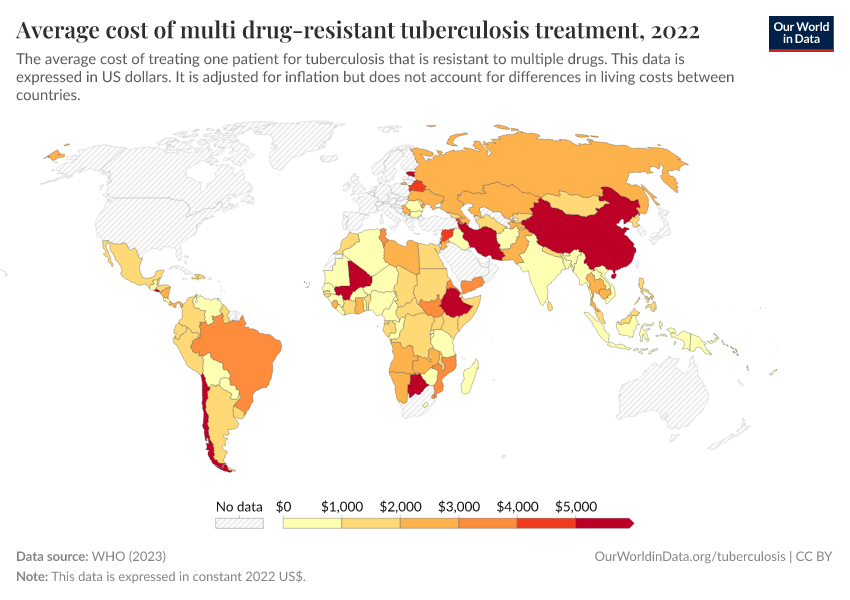
Tuberculosis is still common in many parts of the world
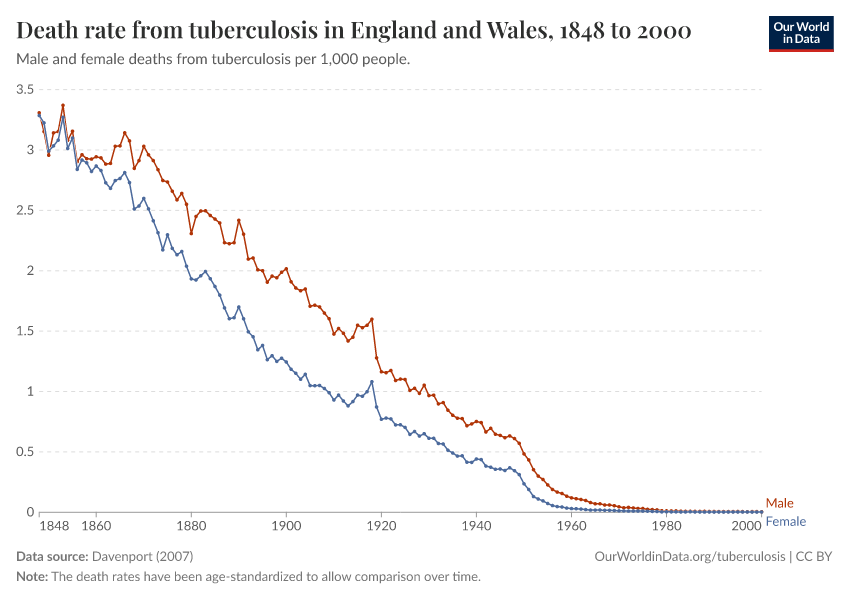
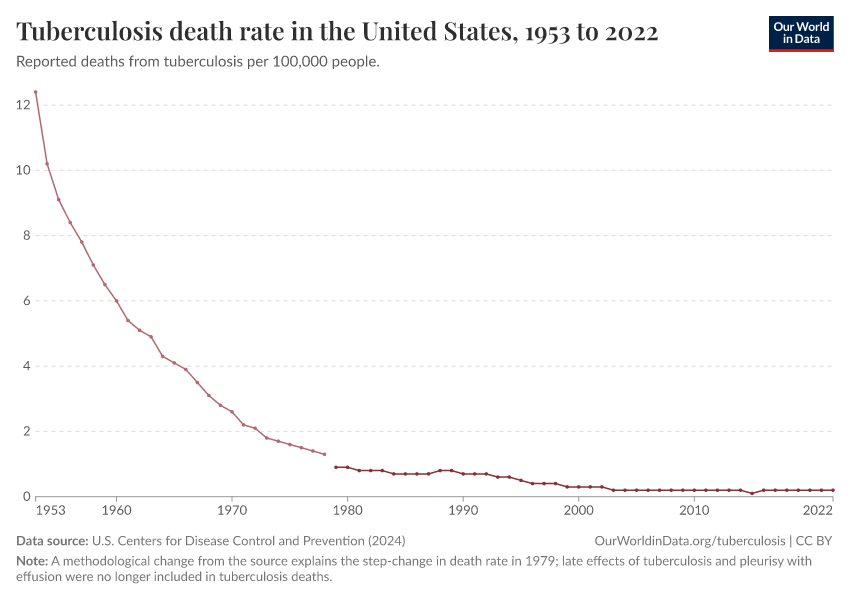
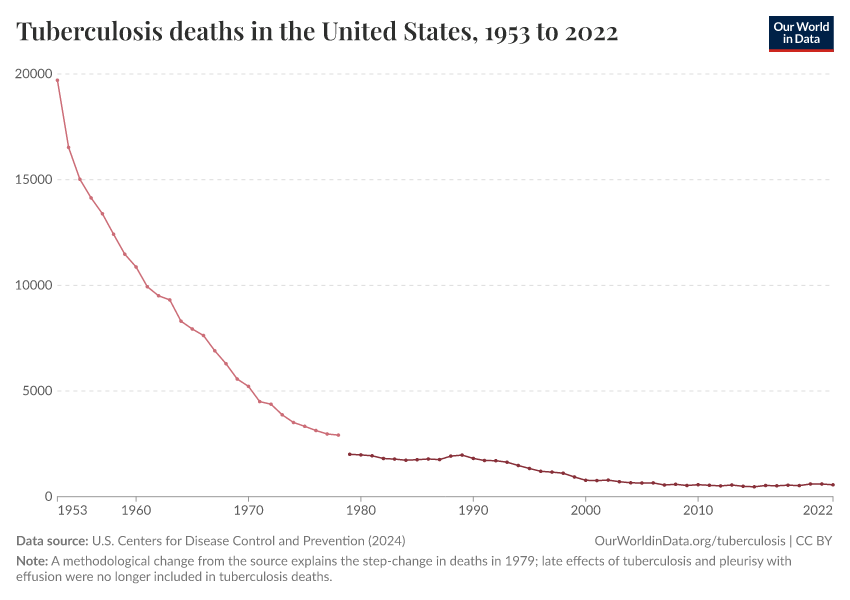
In high-income countries, tuberculosis is largely a disease of the past. Since the beginning of the 20th century, its impact has been significantly reduced with the development of antibiotics and improvements in healthcare and living standards.
But in poorer regions of the world, it is still very common. This makes it one of the most common causes of death from infectious diseases, globally. As you can see on the map, the disease remains common in many countries in Africa, Asia, and South America.
Tuberculosis is highly infectious, and many countries around the world still lack the necessary diagnostic tools and effective medication. This is becoming a bigger challenge as antibiotic resistance has grown.
In addition, many people in affected countries are affected by malnutrition, smoking, occupational risks and overcrowding, and HIV/AIDS, which all increase the risk of developing tuberculosis.1
What you should know about this data
- The World Health Organization relies on mortality data and surveys of tuberculosis prevalence and drug resistance from individual countries. With this data, statistical modeling is used to estimate the incidence of tuberculosis in all countries, as shown on this map.
- For countries where national-level data is lacking for certain years, estimates of changes over time are based on data from neighboring countries.

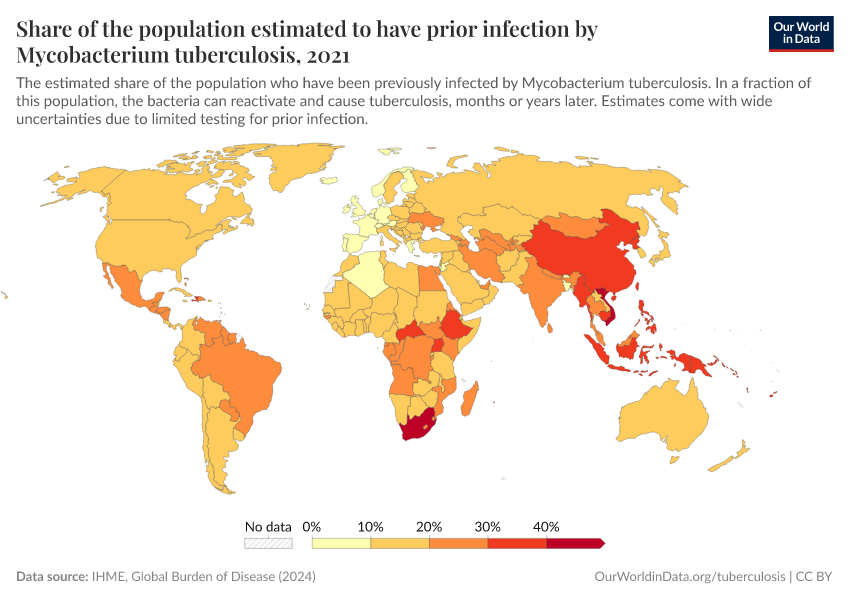
Tuberculosis can cause disease months or years after an infection
Tuberculosis is an infectious disease caused by the bacteria Mycobacterium tuberculosis.
It spreads from people as they breathe, cough, sneeze, shout, or share the bacterial particles in other ways. The bacteria can then infect other people who inhale them.
The diagram shows how the disease can develop within a person over time.
Some people clear the infection quickly.
But others do not, and can develop “active tuberculosis”.
When this happens, they tend to have symptoms such as coughing, fatigue, weight loss, or night sweats, and they become infectious. The disease can cause damage to their lungs, brain, lymphatic system, kidneys, and other organs.
Or, the bacteria can remain “latent” in their body. In this case, people may not have noticeable symptoms and are not infectious – and the infection can be difficult to detect accurately.2
Later on – months or years later – latent tuberculosis can potentially reactivate and turn into active tuberculosis. This happens in a fraction of those with latent tuberculosis, and tends to be more likely if they have a weak immune system from conditions like HIV/AIDS, malnutrition, diabetes, or smoking.3
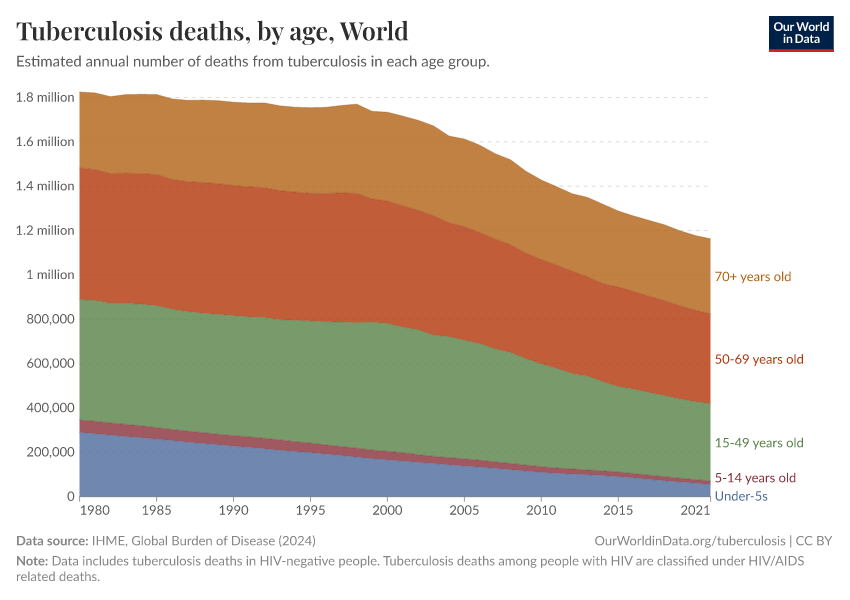
Tuberculosis kills over a million people annually, most of whom are adults
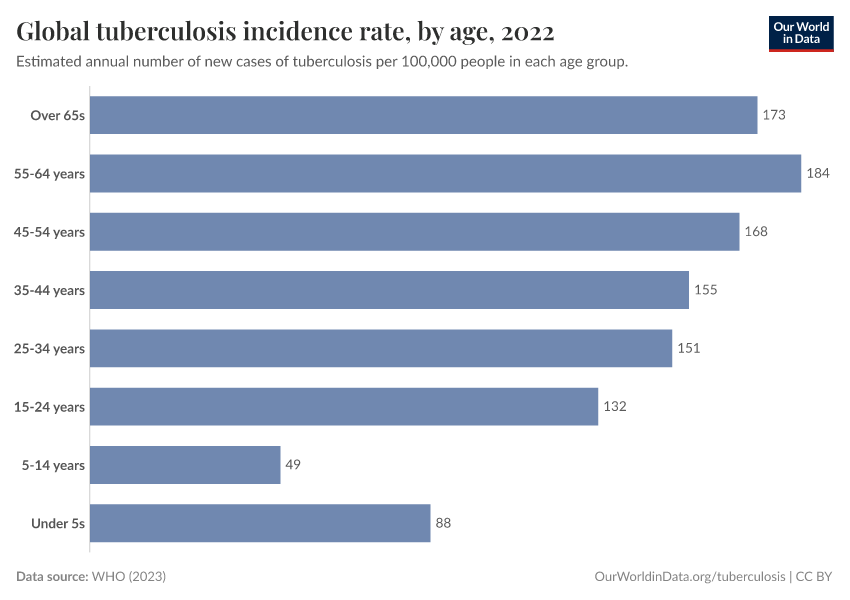
Tuberculosis kills over a million people each year, as you can see in the chart. The chart shows that most of those who die from tuberculosis are adults.4
Its mortality in adults is due to a range of risk factors that make some people more vulnerable to tuberculosis. These include smoking, certain occupations such as nursing and healthcare work, HIV/AIDS, and chronic health conditions.5
In the early 1990s, tuberculosis used to kill around 250,000 children annually. But child deaths from the disease have shrunk as BCG vaccines have become more widely used.
Although the world has had a childhood vaccine against tuberculosis for over a hundred years, a vaccine for adults is still unavailable.6
What you should know about this data
- The estimates made by the source assign each death a single cause based on data on the underlying cause of death listed on death certificates, verbal autopsies, and statistical modeling. This is a simplification, as people often have multiple diseases or injuries that contribute to their death, which may also be listed on death certificates.

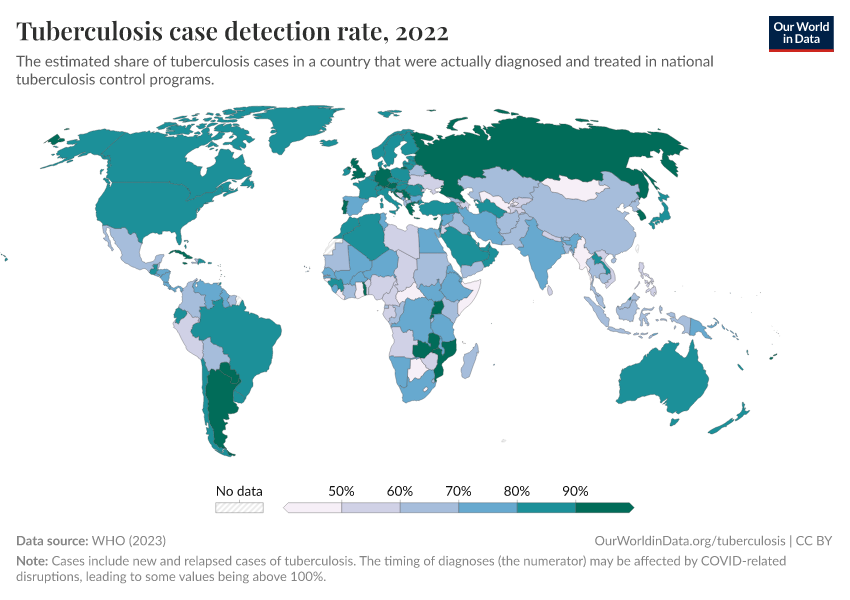
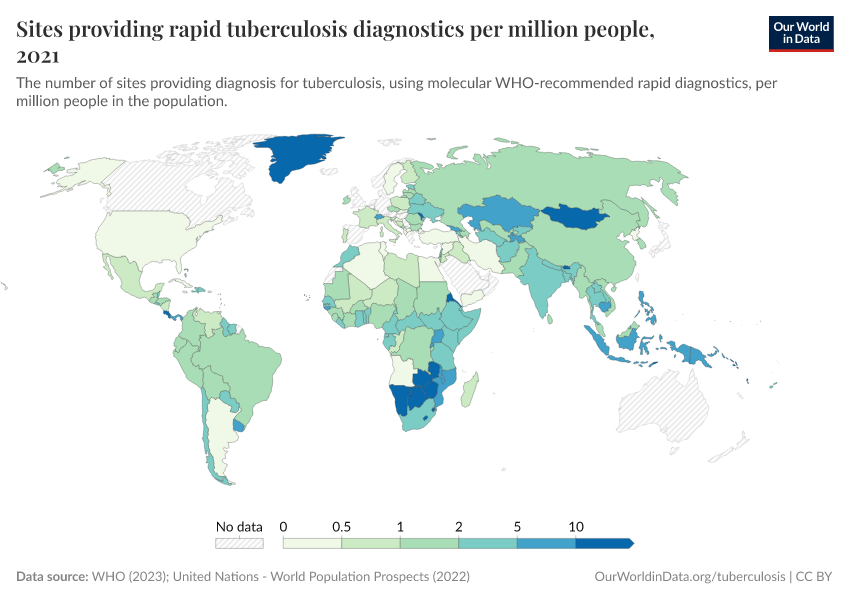
Many people with tuberculosis are undiagnosed
Although tuberculosis is typically a disease of the lungs, the bacteria can affect many organs in the body, and people who are infected don’t always have respiratory symptoms. Instead, they may experience weight loss, breathlessness, fever, or night sweats.
These symptoms are not specific to tuberculosis, so a medical diagnosis is crucial. This may involve skin tests, chest X-rays, blood tests, sputum (spit) tests, or bacterial DNA tests.7
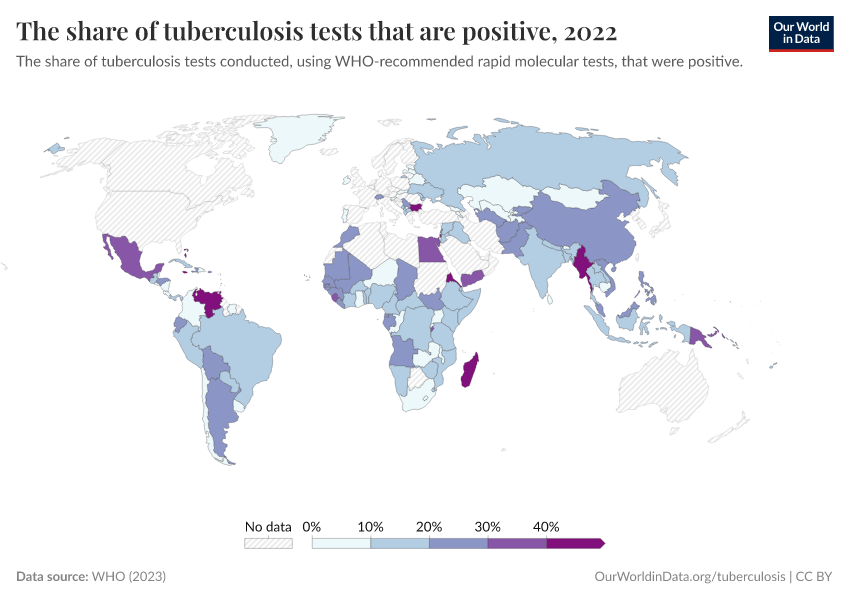
However, the level of testing to diagnose tuberculosis is inadequate in many countries, which means many cases go unnoticed.
The map shows estimates of the share of people with tuberculosis who are diagnosed.
As you can see, case detection rates tend to be lower in countries in Africa and Asia.
Lower rates of diagnosis put people at risk of serious health complications, including the risk of dying from the disease. It also increases the risk that drug-resistant tuberculosis will develop.
What you should know about this data
- The tuberculosis detection rate is a fraction. The numerator is the annual number of diagnosed active tuberculosis cases from each country. The denominator is the estimated annual number of active tuberculosis cases in the country based on national data and statistical modeling.
- To estimate the annual number of cases, the researchers rely on mortality data and surveys of prevalence and drug resistance from individual countries. With this data, statistical modeling is used to estimate the incidence of tuberculosis in countries and regions over time.
- For countries where national-level data is lacking for certain years, estimates of changes over time are based on regional data.

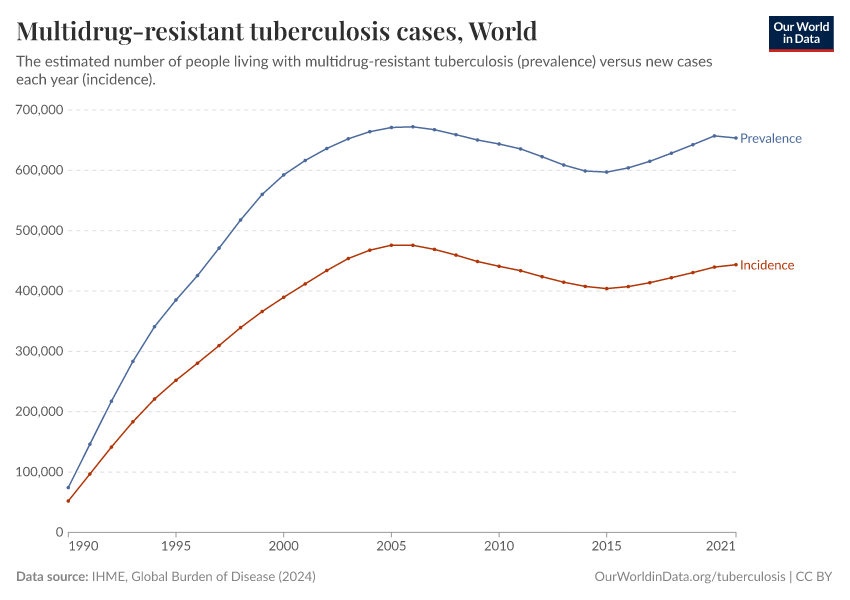
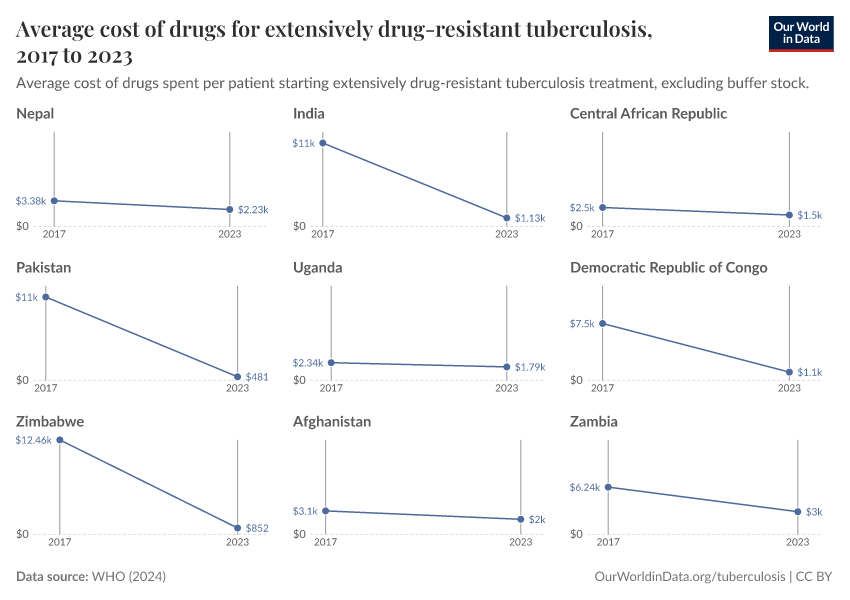
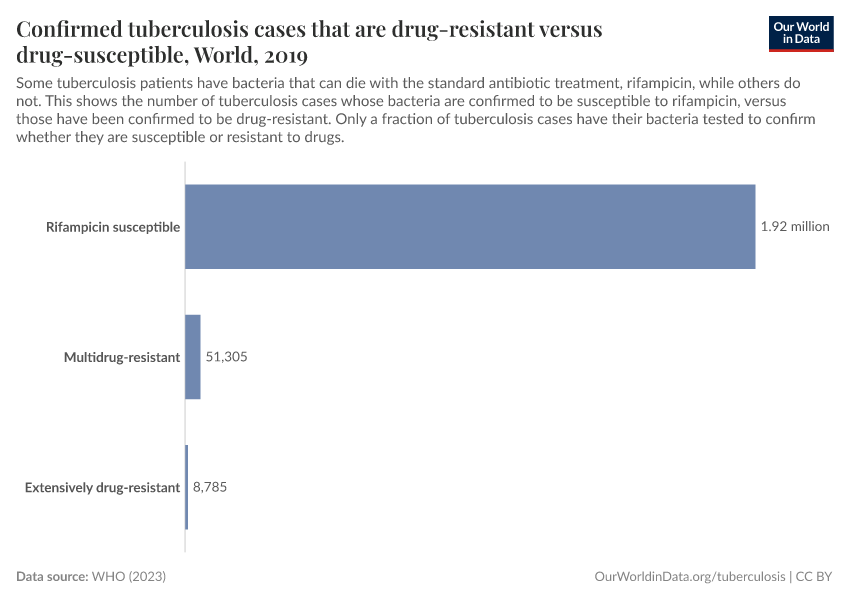
Antibiotic resistance is an important consideration during treatment
People with tuberculosis require treatment with a specific combination of antibiotic medications that can kill the bacteria.
Without proper treatment, the bacteria can survive and potentially develop antibiotic resistance.
This drug-resistant bacteria can then spread to others, causing infections that are much more difficult and expensive to treat, and their treatments can have more side effects.8
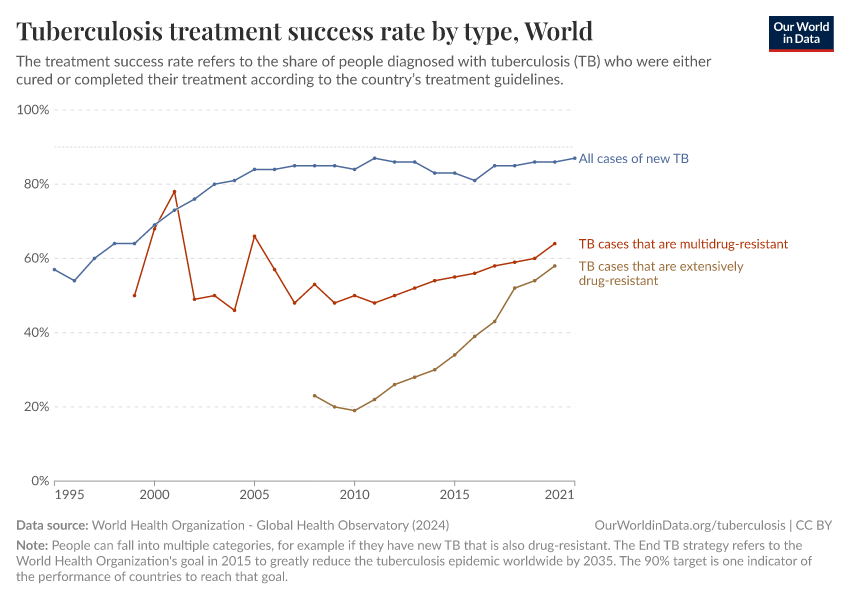
The chart shows the “treatment success rate” among people with tuberculosis – those who have been cured or have completed the whole course of treatment. This is compared between all new cases of tuberculosis versus those with drug-resistant tuberculosis.
You can see that drug-resistant tuberculosis, especially excessively drug-resistant tuberculosis, has a lower treatment success rate.
In recent years, there has been some improvement in the treatment success rate of people with drug-resistant tuberculosis – with better testing, new guidelines on using antibiotic treatment appropriately, and new drugs – but there is still more progress that can be achieved.9
What you should know about this data
- Only a fraction of tuberculosis cases are tested for drug resistance. Drug resistance is tested using rapid molecular tests, culture methods, or sequencing technologies.

HIV increases the risk of developing tuberculosis
An HIV infection is a major risk factor for developing tuberculosis.10
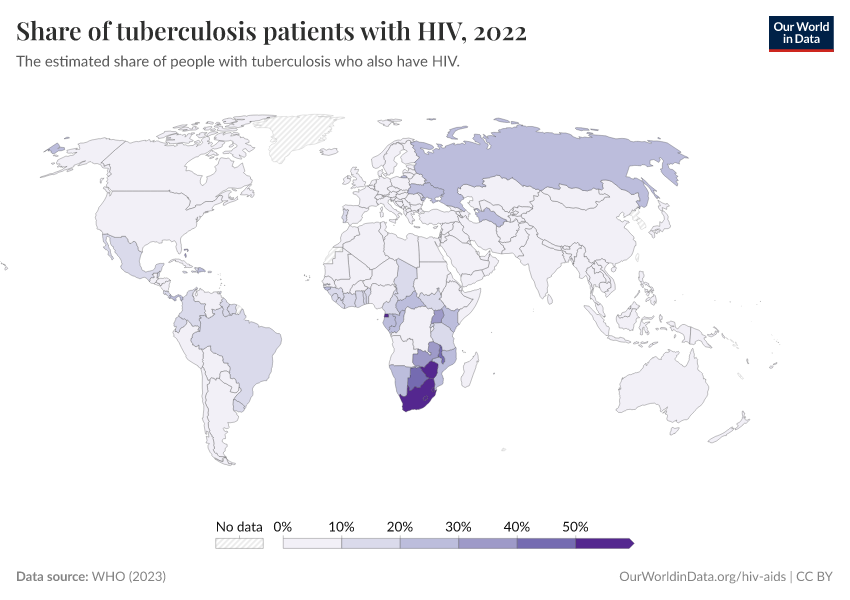
The map shows the estimated share of tuberculosis patients who also have HIV.
You can see that there are multiple countries in southern Africa – such as South Africa, Zimbabwe and Botswana – where a significant share of those with tuberculosis also have HIV.
As HIV weakens the immune system, the tuberculosis bacteria can thrive and can cause more serious lung disease. This impact is large, and tuberculosis is a major cause of death in people with HIV/AIDS.11
In parallel, tuberculosis infections can speed up the multiplication of the HIV virus, which quickens the development of AIDS and leads to a rapid deterioration in health.10
What you should know about this data
- Data on tuberculosis comes from mortality data and surveys of prevalence and drug resistance from individual countries. With this data, statistical modeling is used to estimate the incidence of tuberculosis in countries and regions over time.
- For countries where national-level data is lacking for certain years, estimates of changes over time are based on regional data.
- Data on HIV comes from observations and statistical modeling based on characteristics of the virus’s transmission, behavioral and clinical data, the availability of treatment, and mortality data from countries with high-quality death registration.

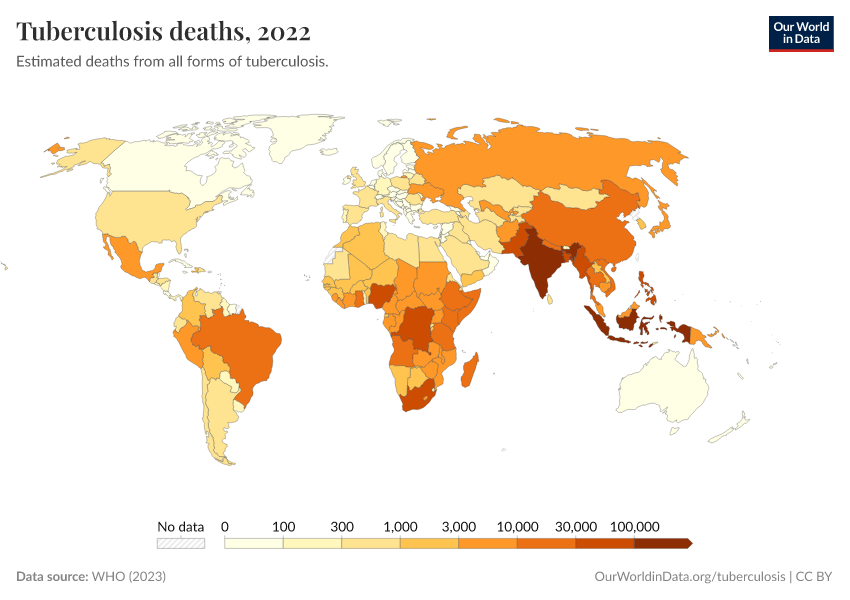
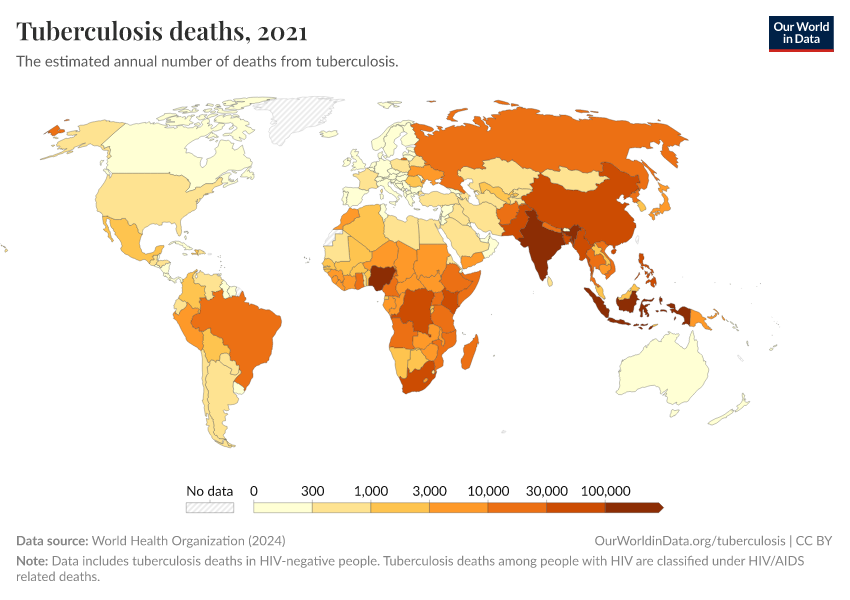
More progress can be made against childhood tuberculosis
Tuberculosis tends to be serious in children because their underdeveloped immune systems make them more vulnerable to the disease, especially if they are undernourished.
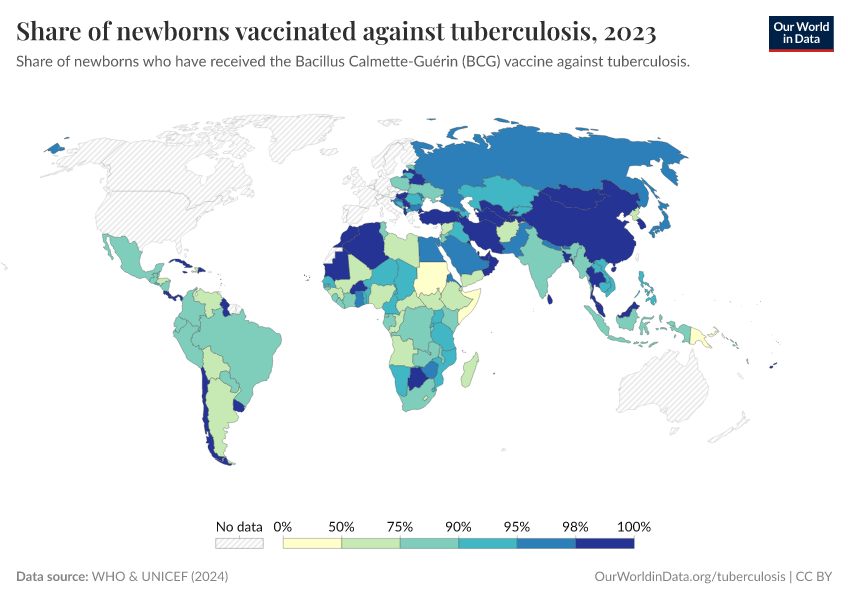
The BCG (Bacillus Calmette-Guérin) vaccine was developed by Albert Calmette and Camille Guérin in 1921 to protect infants and young children from severe tuberculosis. Since then, it has become one of the most widely used childhood vaccines worldwide.
Yet, as the map shows, tens of thousands of children still die from the disease, and it is one of the major causes of death in children.
One reason is that the vaccine’s efficacy tends to be lower in some parts of the world.12
Children also remain at risk for other reasons: for example, there is a lack of medication and diagnostic testing developed for children. In addition, many children, especially in Africa, also suffer from HIV/AIDS, which makes them more vulnerable to tuberculosis.13
What you should know about this data
- The estimates made by the source assign each death a single cause based on data on the underlying cause of death listed on death certificates, verbal autopsies, and statistical modeling. This is a simplification, as people often have multiple diseases or injuries that contribute to their death, which may also be listed on death certificates.

Research & Writing
July 28, 2025
The world left its fight against tuberculosis unfinished — how can we complete the job?
If we get it right, the world could save more than 1.2 million lives every year.
June 2, 2025
Once a leading killer, tuberculosis is now rare in rich countries — here’s how it happened
As much as one quarter of deaths in Europe and the United States were once from tuberculosis.
More articles on tuberculosis
Key Charts on Tuberculosis
See all charts on this topic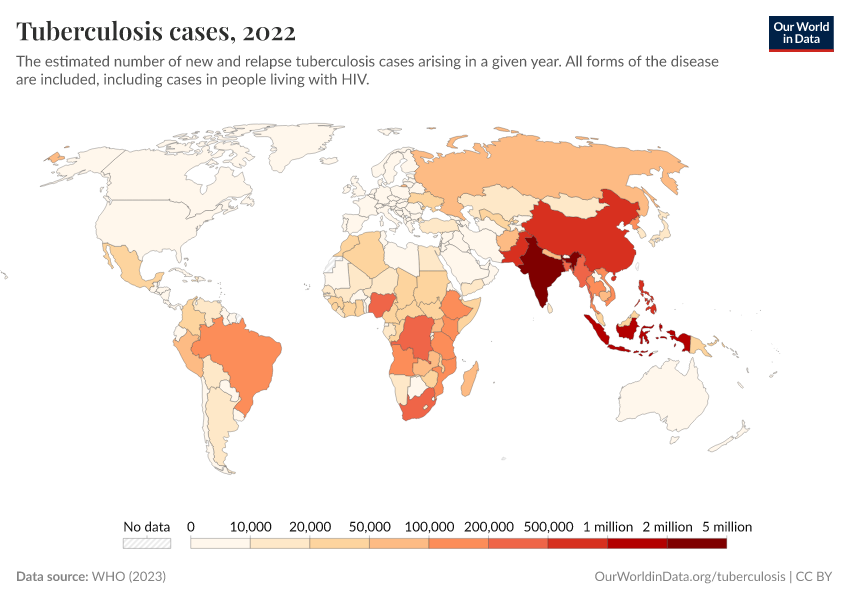









































Featured Data on Tuberculosis
Endnotes
Floyd, K., Glaziou, P., Zumla, A., & Raviglione, M. (2018). The global tuberculosis epidemic and progress in care, prevention, and research: An overview in year 3 of the End TB era. The Lancet Respiratory Medicine, 6(4), 299–314. https://doi.org/10.1016/S2213-2600(18)30057-2
Fukunaga, R., Glaziou, P., Harris, J. B., Date, A., Floyd, K., & Kasaeva, T. (2021). Epidemiology of Tuberculosis and Progress Toward Meeting Global Targets—Worldwide, 2019. MMWR. Morbidity and Mortality Weekly Report, 70(12), 427–430. https://doi.org/10.15585/mmwr.mm7012a4
Glaziou, P., Floyd, K., & Raviglione, M. (2018). Global Epidemiology of Tuberculosis. Seminars in Respiratory and Critical Care Medicine, 39(03), 271–285. https://doi.org/10.1055/s-0038-1651492
Esmail, H., Barry, C. E., Young, D. B., & Wilkinson, R. J. (2014). The ongoing challenge of latent tuberculosis. Philosophical Transactions of the Royal Society B: Biological Sciences, 369(1645), 20130437. https://doi.org/10.1098/rstb.2013.0437
Horton, K. C., Richards, A. S., Emery, J. C., Esmail, H., & Houben, R. M. G. J. (2023). Reevaluating progression and pathways following Mycobacterium tuberculosis infection within the spectrum of tuberculosis. Proceedings of the National Academy of Sciences, 120(47), e2221186120. https://doi.org/10.1073/pnas.2221186120
Migliori, G. B., & Raviglione, M. C. (Eds.). (2021). Essential Tuberculosis. Springer International Publishing. https://doi.org/10.1007/978-3-030-66703-0
Shah, M., & Dorman, S. E. (2021). Latent Tuberculosis Infection. New England Journal of Medicine, 385(24), 2271–2280. https://doi.org/10.1056/NEJMcp2108501
Zellweger, J. P., Sotgiu, G., Corradi, M., & Durando, P. (2020). The diagnosis of latent tuberculosis infection (LTBI): Currently available tests, future developments, and perspectives to eliminate tuberculosis (TB): The diagnosis of latent tuberculosis infection (LTBI). La Medicina Del Lavoro | Work, Environment and Health, 111(3), 170–183. https://doi.org/10.23749/mdl.v111i3.9983
Churchyard, G., Kim, P., Shah, N. S., Rustomjee, R., Gandhi, N., Mathema, B., Dowdy, D., Kasmar, A., & Cardenas, V. (2017). What We Know About Tuberculosis Transmission: An Overview. The Journal of Infectious Diseases, 216(suppl_6), S629–S635. https://doi.org/10.1093/infdis/jix362
Mathema, B., Andrews, J. R., Cohen, T., Borgdorff, M. W., Behr, M., Glynn, J. R., Rustomjee, R., Silk, B. J., & Wood, R. (2017). Drivers of Tuberculosis Transmission. The Journal of Infectious Diseases, 216(suppl_6), S644–S653. https://doi.org/10.1093/infdis/jix354
In addition, some people who have had active tuberculosis can then develop latent tuberculosis, which can later reactivate again, causing a recurrence of the disease.
Rates of tuberculosis also tend to be higher among adults.
Amere, G. A., Nayak, P., Salindri, A. D., Narayan, K. M. V., & Magee, M. J. (2018). Contribution of Smoking to Tuberculosis Incidence and Mortality in High-Tuberculosis-Burden Countries. American Journal of Epidemiology, 187(9), 1846–1855. https://doi.org/10.1093/aje/kwy081
Bell, L. C. K., & Noursadeghi, M. (2018). Pathogenesis of HIV-1 and Mycobacterium tuberculosis co-infection. Nature Reviews Microbiology, 16(2), 80–90. https://doi.org/10.1038/nrmicro.2017.128
Bruchfeld, J., Correia-Neves, M., & Källenius, G. (2015). Tuberculosis and HIV Coinfection. Cold Spring Harbor Perspectives in Medicine, 5(7), a017871. https://doi.org/10.1101/cshperspect.a017871
Uden, L., Barber, E., Ford, N., & Cooke, G. S. (2017). Risk of Tuberculosis Infection and Disease for Health Care Workers: An Updated Meta-Analysis. Open Forum Infectious Diseases, 4(3), ofx137. https://doi.org/10.1093/ofid/ofx137
Schrager, L. K., Vekemens, J., Drager, N., Lewinsohn, D. M., & Olesen, O. F. (2020). The status of tuberculosis vaccine development. The Lancet Infectious Diseases, 20(3), e28–e37. https://doi.org/10.1016/S1473-3099(19)30625-5
Migliori, G. B., & Raviglione, M. C. (Eds.). (2021). Essential Tuberculosis. Springer International Publishing. https://doi.org/10.1007/978-3-030-66703-0
This is especially a problem for tuberculosis because many treatments for the disease need to be taken for several months. This is for two reasons: the bacteria have more time to develop resistance, and it makes it more likely that people do not continue to follow the prescriptions, which makes it easier for bacteria to develop resistance.
Lange, C., Dheda, K., Chesov, D., Mandalakas, A. M., Udwadia, Z., & Horsburgh, C. R. (2019). Management of drug-resistant tuberculosis. The Lancet, 394(10202), 953–966. https://doi.org/10.1016/S0140-6736(19)31882-3
Gygli, S. M., Borrell, S., Trauner, A., & Gagneux, S. (2017). Antimicrobial resistance in Mycobacterium tuberculosis: Mechanistic and evolutionary perspectives. FEMS Microbiology Reviews, 41(3), 354–373. https://doi.org/10.1093/femsre/fux011
World Health Organization. (2015). The end TB strategy. https://web.archive.org/web/20231214163433/https://iris.who.int/bitstream/handle/10665/331326/WHO-HTM-TB-2015.19-eng.pdf
World Health Organization (2019). WHO consolidated guidelines on drug-resistant tuberculosis treatment. Available online. https://iris.who.int/bitstream/handle/10665/311389/9789241550529-eng.pdf
Kendall, E. A., Sahu, S., Pai, M., Fox, G. J., Varaine, F., Cox, H., Cegielski, J. P., Mabote, L., Vassall, A., & Dowdy, D. W. (2019). What will it take to eliminate drug-resistant tuberculosis? The International Journal of Tuberculosis and Lung Disease, 23(5), 535–546. https://doi.org/10.5588/ijtld.18.0217
Bell, L. C. K., & Noursadeghi, M. (2018). Pathogenesis of HIV-1 and Mycobacterium tuberculosis co-infection. Nature Reviews Microbiology, 16(2), 80–90. https://doi.org/10.1038/nrmicro.2017.128
Bruchfeld, J., Correia-Neves, M., & Källenius, G. (2015). Tuberculosis and HIV Coinfection. Cold Spring Harbor Perspectives in Medicine, 5(7), a017871. https://doi.org/10.1101/cshperspect.a017871
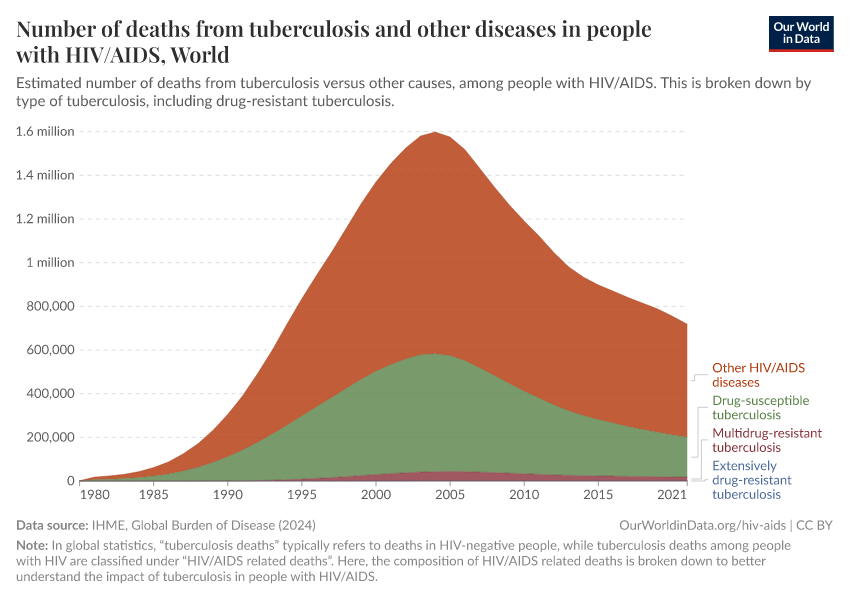
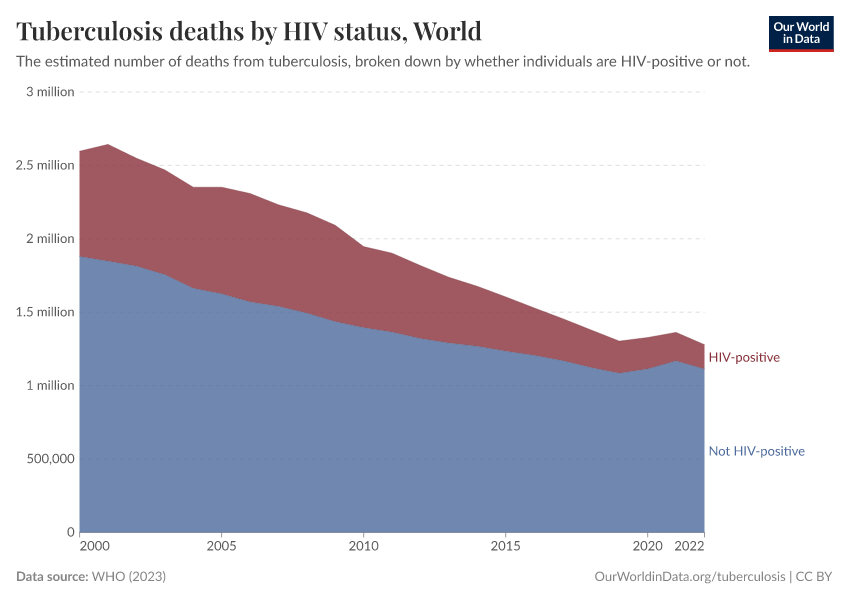
HIV/AIDS makes people vulnerable to multiple diseases which can be fatal, including tuberculosis.
Typically, in international statistics, “tuberculosis deaths” refers to deaths in HIV-negative people, while tuberculosis deaths among people with HIV are classified under “HIV/AIDS related deaths”.
Here, the composition of HIV/AIDS related deaths are broken down to better understand the impact of tuberculosis among people with HIV/AIDS.
The BCG vaccine’s efficacy varies between locations and is generally found to be more effective in countries far from the equator.
This is likely due to a range of factors, such as different strains of Mycobacterium tuberculosis around the world; exposure to other mycobacteria in the environment, which can affect the immune system’s response to the vaccine; and other factors.
Cirillo, D. M., Ghodousi, A., & Tortoli, E. (2021). Mycobacterium tuberculosis: The Organism’s Genomics and Evolution. In G. B. Migliori & M. C. Raviglione (Eds.), Essential Tuberculosis (pp. 11–17). Springer International Publishing. https://doi.org/10.1007/978-3-030-66703-0_2
Fatima, S., Kumari, A., Das, G., & Dwivedi, V. P. (2020). Tuberculosis vaccine: A journey from BCG to present. Life Sciences, 252, 117594. https://doi.org/10.1016/j.lfs.2020.117594
Kuan, R., Muskat, K., Peters, B., & Lindestam Arlehamn, C. S. (2020). Is mapping the BCG vaccine‐induced immune responses the key to improving the efficacy against tuberculosis? Journal of Internal Medicine, 288(6), 651–660. https://doi.org/10.1111/joim.13191
In addition, children who suffer from HIV are not recommended to take the BCG vaccine.
Carvalho, A. C. C., Cardoso, C. A. A., Martire, T. M., Migliori, G. B., & Sant’Anna, C. C. (2018). Epidemiological aspects, clinical manifestations, and prevention of pediatric tuberculosis from the perspective of the End TB Strategy. Jornal Brasileiro de Pneumologia, 44(2), 134–144. https://doi.org/10.1590/s1806-37562017000000461
Swaminathan, S., & Rekha, B. (2010). Pediatric Tuberculosis: Global Overview and Challenges. Clinical Infectious Diseases, 50(s3), S184–S194. https://doi.org/10.1086/651490
Cite this work
Our articles and data visualizations rely on work from many different people and organizations. When citing this topic page, please also cite the underlying data sources. This topic page can be cited as:
Saloni Dattani, Fiona Spooner, Hannah Ritchie, and Max Roser (2023) - “Tuberculosis” Published online at OurWorldinData.org. Retrieved from: 'https://ourworldindata.org/tuberculosis' [Online Resource]BibTeX citation
@article{owid-tuberculosis,
author = {Saloni Dattani and Fiona Spooner and Hannah Ritchie and Max Roser},
title = {Tuberculosis},
journal = {Our World in Data},
year = {2023},
note = {https://ourworldindata.org/tuberculosis}
}Reuse this work freely
All visualizations, data, and articles produced by Our World in Data are completely open access under the Creative Commons BY license. You have the permission to use, distribute, and reproduce these in any medium, provided the source and authors are credited.
The data produced by third parties and made available by Our World in Data is subject to the license terms from the original third-party authors. We will always indicate the original source of the data in our documentation, so you should always check the license of any such third-party data before use and redistribution.
All of our charts can be embedded in any site.