Mental Health
Mental health is an essential part of people’s lives and society. Poor mental health affects our well-being, our ability to work, and our relationships with friends, family, and community.
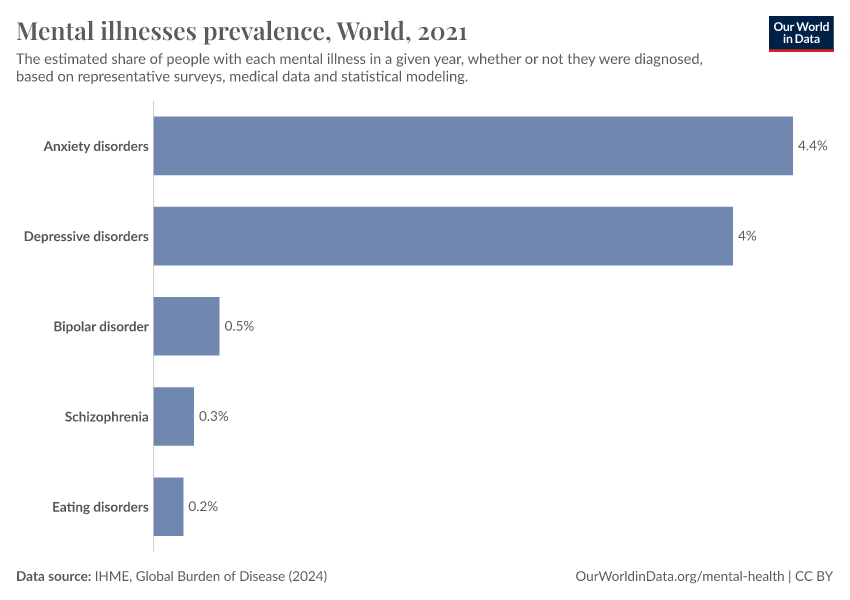
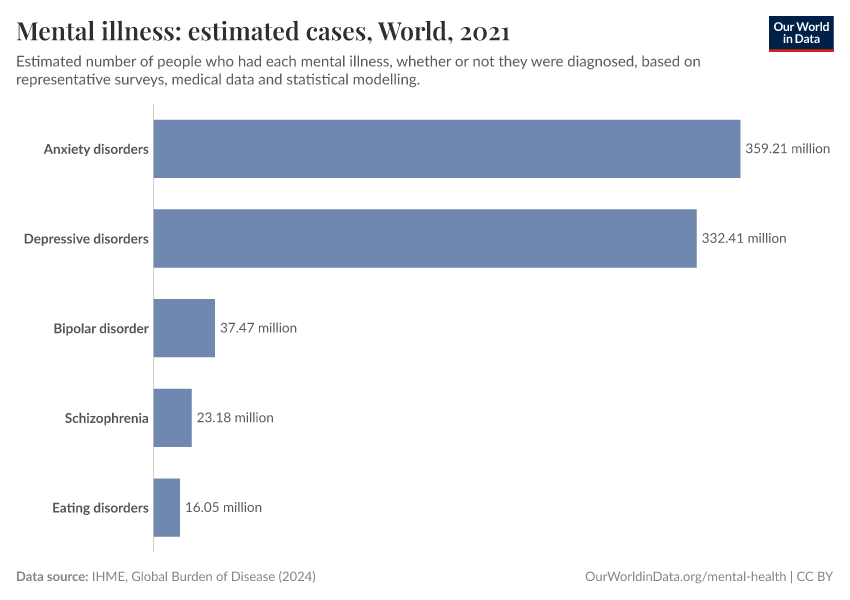
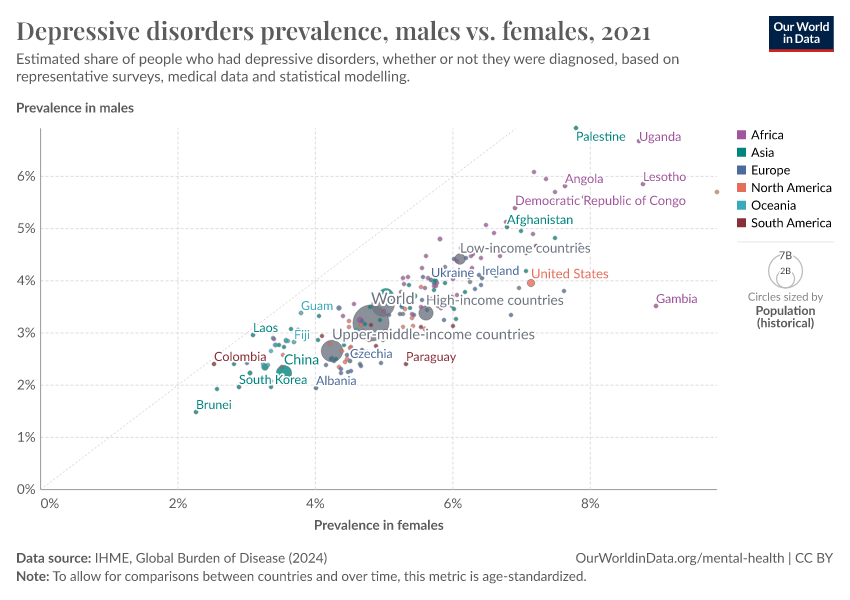
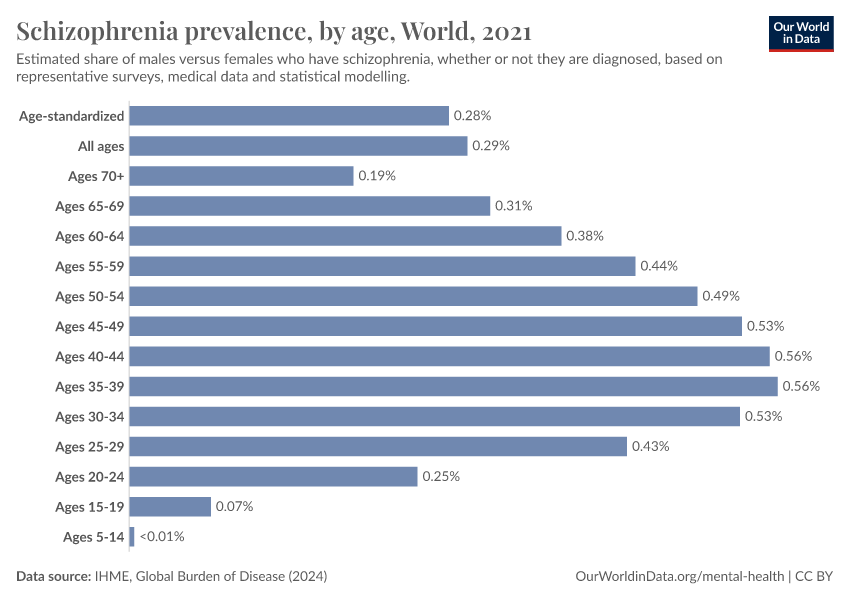
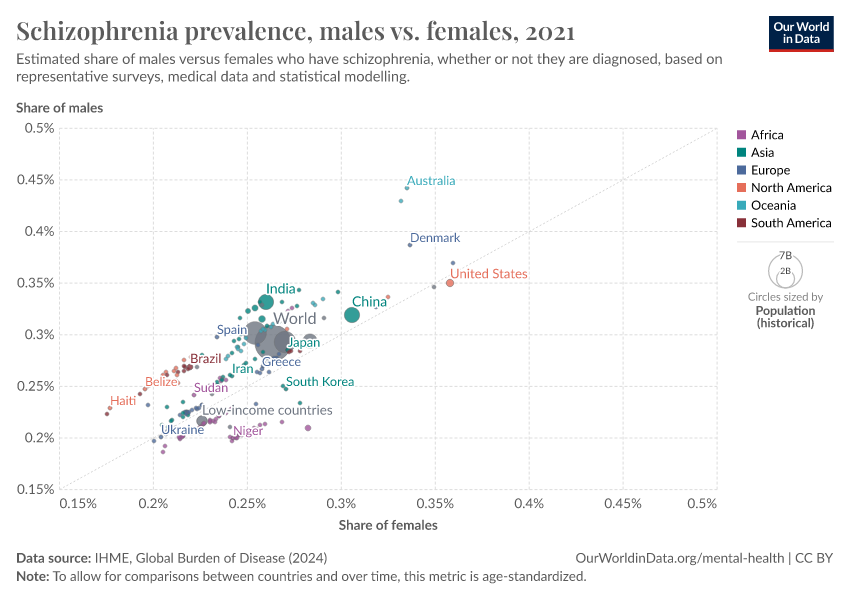
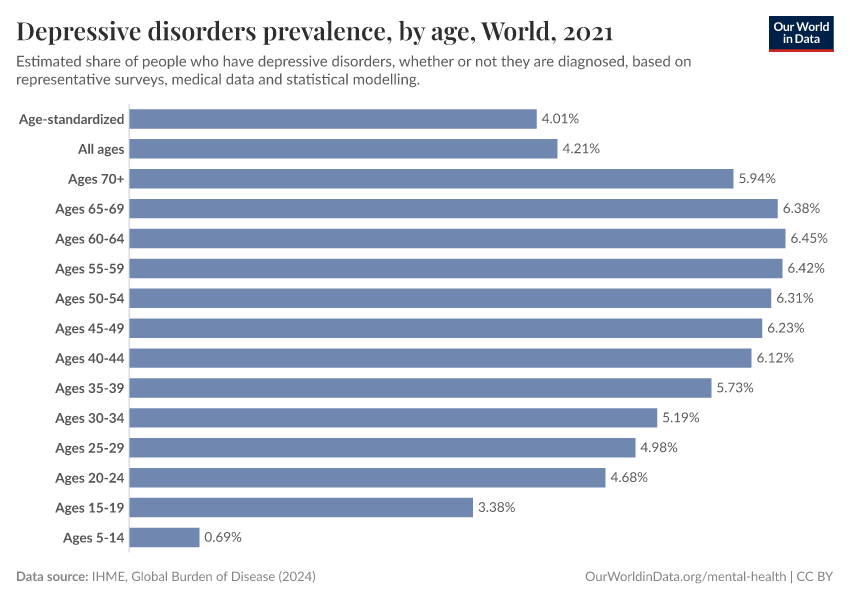
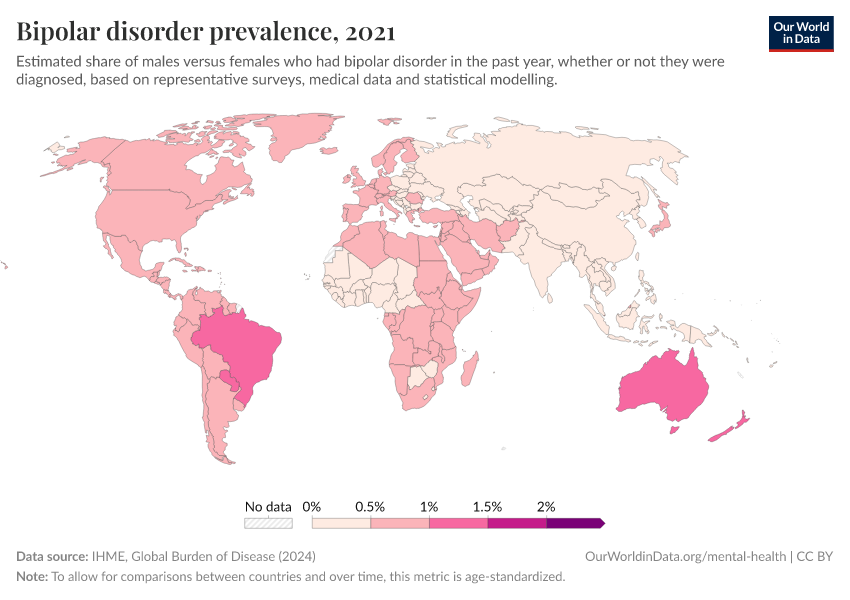
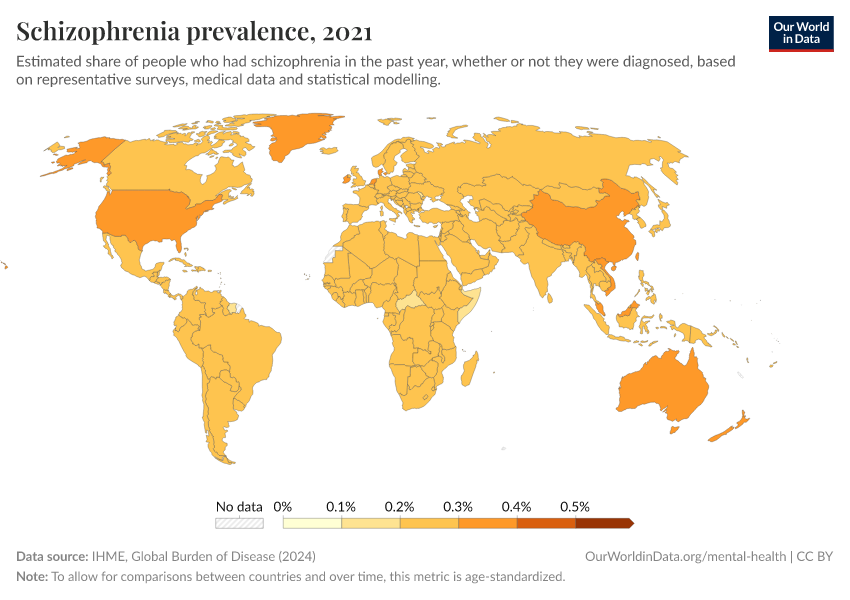
Mental health conditions are not uncommon. Hundreds of millions suffer from them yearly, and many more do over their lifetimes. It’s estimated that 1 in 3 women and 1 in 5 men will experience major depression in their lives. Other conditions, such as schizophrenia and bipolar disorder, are less common but still have a large impact on people’s lives.
Mental illnesses are treatable, and the impact they have can be reduced. Despite this, treatment is often lacking or poor quality, and many feel uncomfortable sharing their symptoms with healthcare professionals or people they know. This also makes it difficult to estimate the actual prevalence of mental illnesses.
To support them, it’s essential to have good data to understand these conditions – how, when, and why they occur, how many people are affected by them, and how they can be treated effectively and safely.
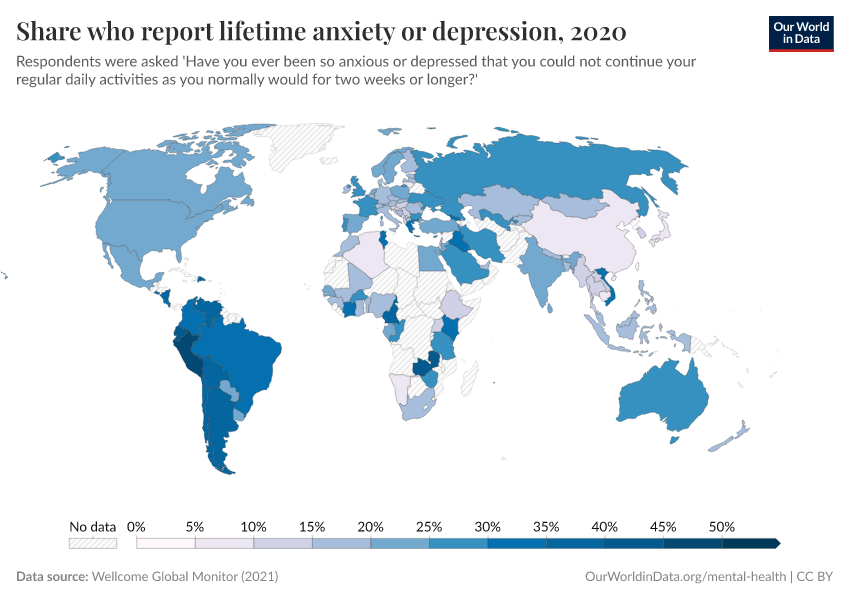
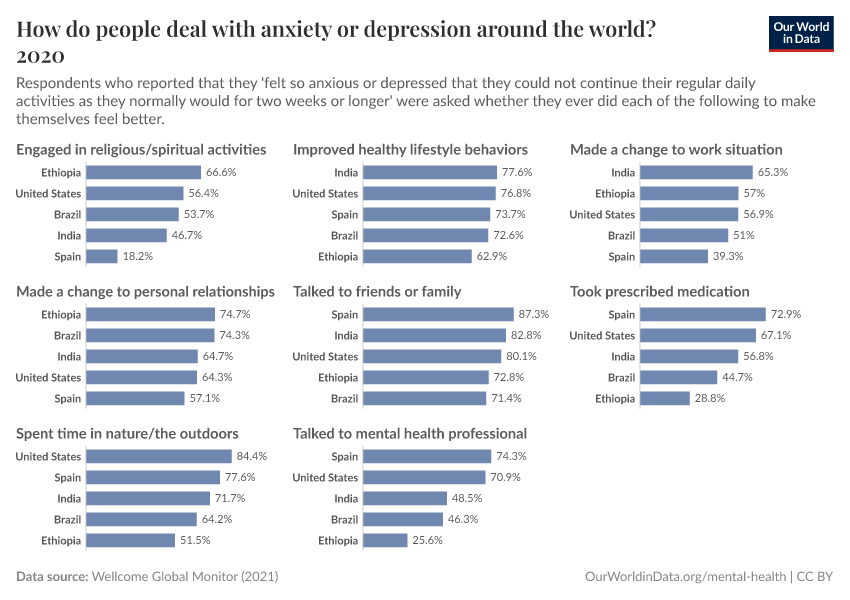
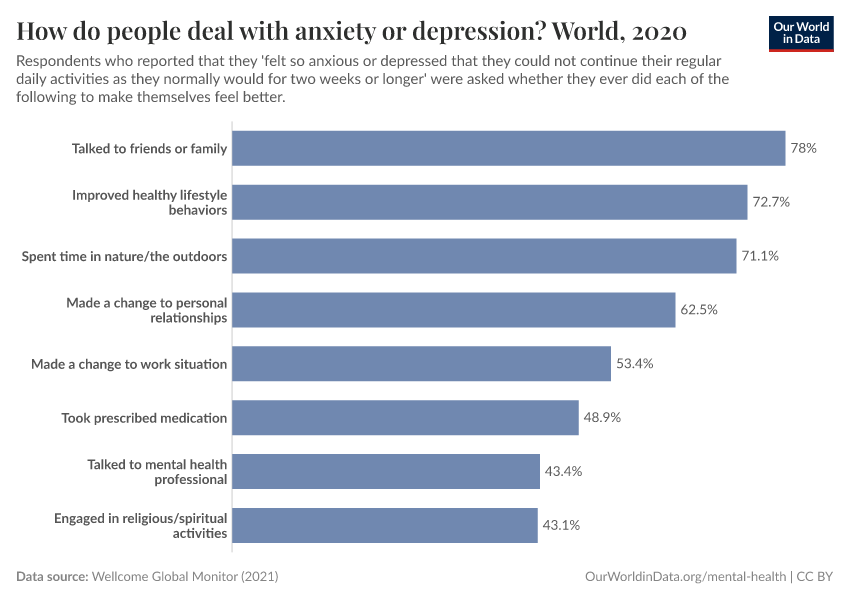
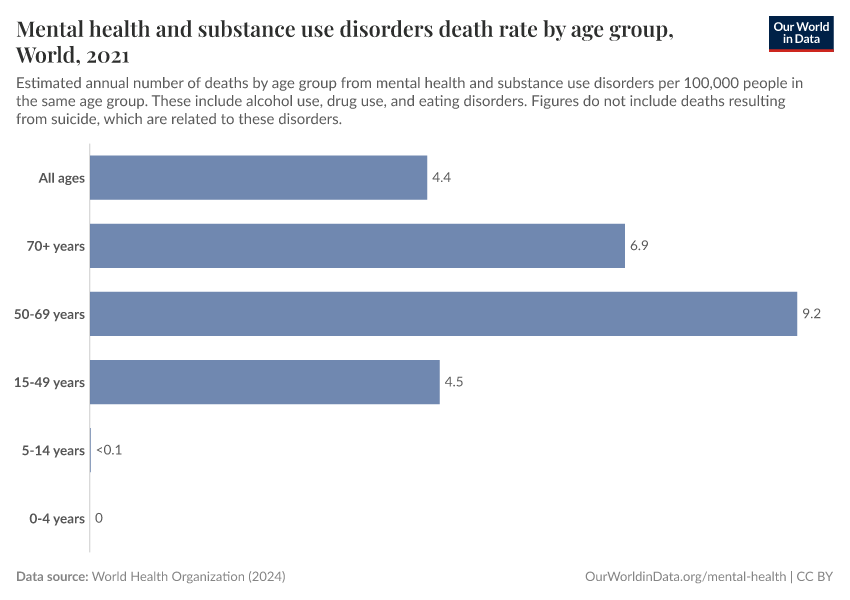
On this page, we show data on the prevalence of mental illnesses and their burden, and people’s attitudes toward mental health.
Research & Writing
May 26, 2023
How do researchers study the prevalence of mental illnesses?
Global data on mental health is essential to understand the scale and patterns of these illnesses, and how to reduce them. How do researchers collect this data, and how reliable is it?
May 26, 2023
How are mental illnesses defined?
Mental illnesses are a range of conditions that significantly affect people’s lives. What are their symptoms?
More articles on Mental Health
November 10, 2025
Anxiety is one of the world’s most common health issues. How have treatments evolved over the last 70 years?
August 26, 2024
Antipsychotic medications: a timeline of innovations and remaining challenges
May 18, 2022
What is the lifetime risk of depression?
April 7, 2022
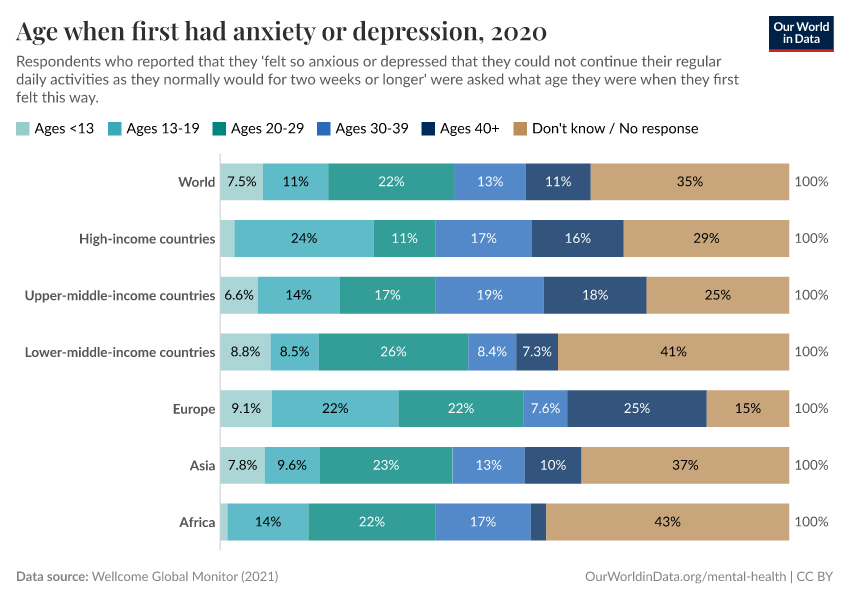
At what age do people experience depression for the first time?
September 1, 2021
Depression is complicated — this is how our understanding of the condition has evolved over time
Key Charts on Mental Health
See all charts on this topic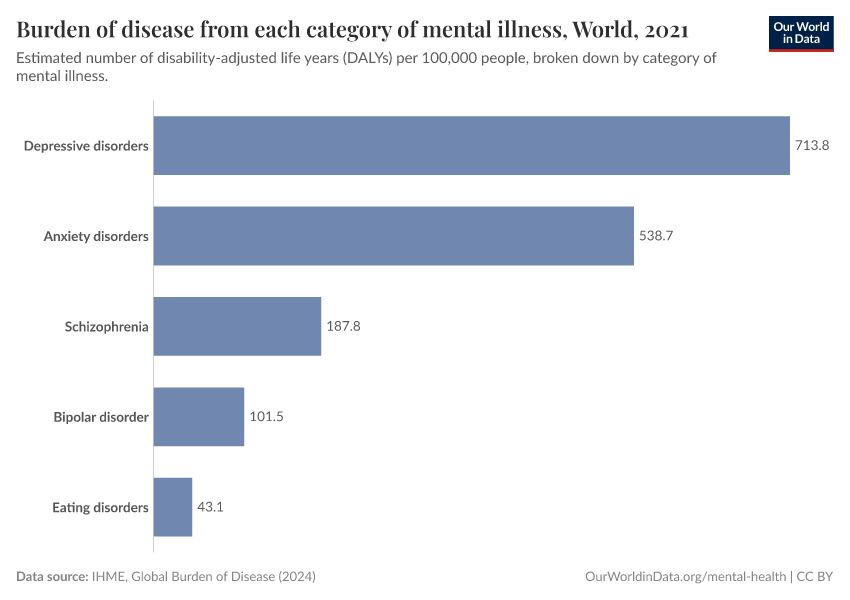



















































Featured Data on Mental Health
Cite this work
Our articles and data visualizations rely on work from many different people and organizations. When citing this topic page, please also cite the underlying data sources. This topic page can be cited as:
Saloni Dattani, Lucas Rodés-Guirao, Hannah Ritchie, and Max Roser (2023) - “Mental Health” Published online at OurWorldinData.org. Retrieved from: 'https://ourworldindata.org/mental-health' [Online Resource]BibTeX citation
@article{owid-mental-health,
author = {Saloni Dattani and Lucas Rodés-Guirao and Hannah Ritchie and Max Roser},
title = {Mental Health},
journal = {Our World in Data},
year = {2023},
note = {https://ourworldindata.org/mental-health}
}Reuse this work freely
All visualizations, data, and articles produced by Our World in Data are completely open access under the Creative Commons BY license. You have the permission to use, distribute, and reproduce these in any medium, provided the source and authors are credited.
The data produced by third parties and made available by Our World in Data is subject to the license terms from the original third-party authors. We will always indicate the original source of the data in our documentation, so you should always check the license of any such third-party data before use and redistribution.
All of our charts can be embedded in any site.