Diarrheal Diseases
Diarrheal diseases are among the most common causes of death, especially in children.
In 2021, around 1.2 million people died from diarrheal diseases. That was equivalent to all violent deaths combined.1
Around 390,000 of these deaths were among children and adolescents.
In recent decades, deaths from diarrheal diseases have fallen significantly across the world as a result of public health interventions. But more progress is possible.
Diarrheal deaths are preventable because they are primarily caused by pathogens, whose spread can be easily controlled.
By increasing global access to clean water and sanitation, oral rehydration therapy, and vaccination, this major cause of death can be reduced substantially.
This page shows estimates of diarrheal death rates worldwide and the pathogens that cause them. We also offer data on access to public health measures and how they have changed.
Key Insights on Diarrheal Diseases
Diarrheal diseases are a leading cause of death among children
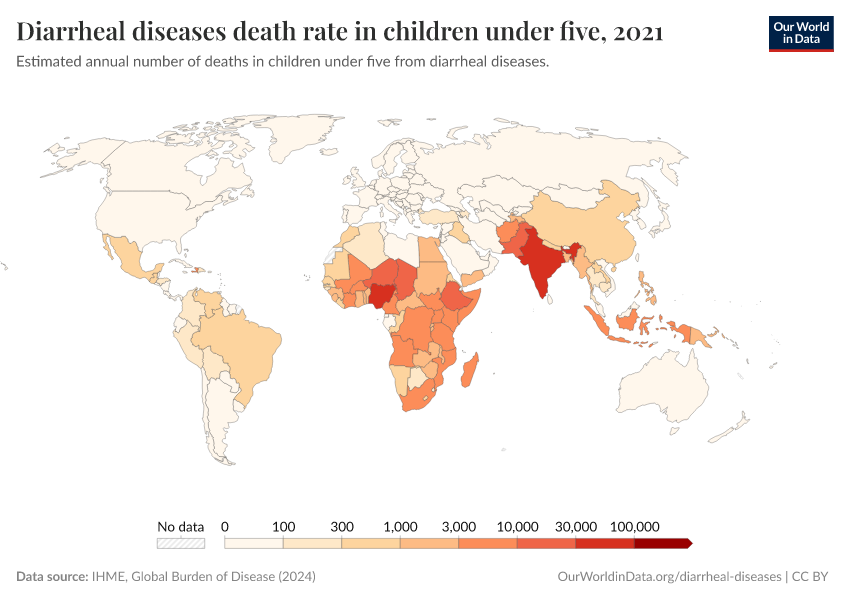
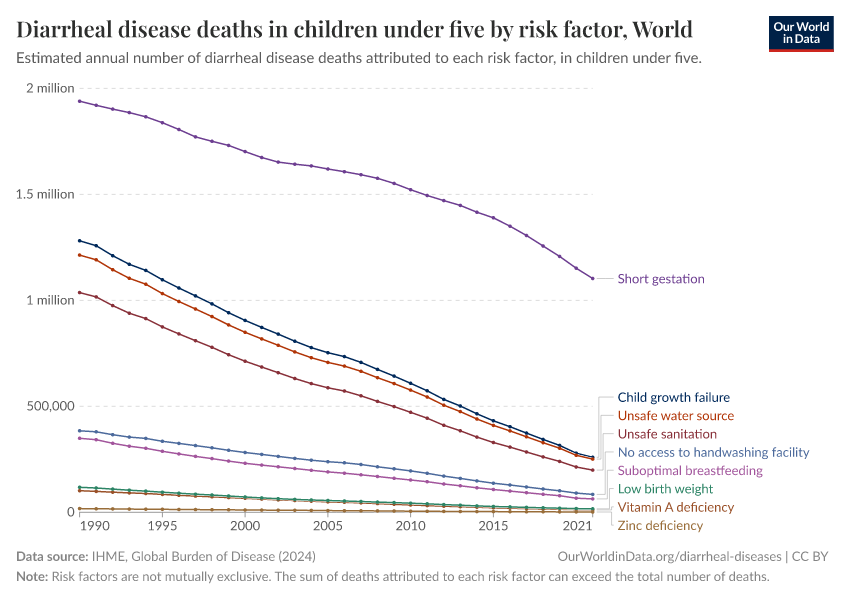
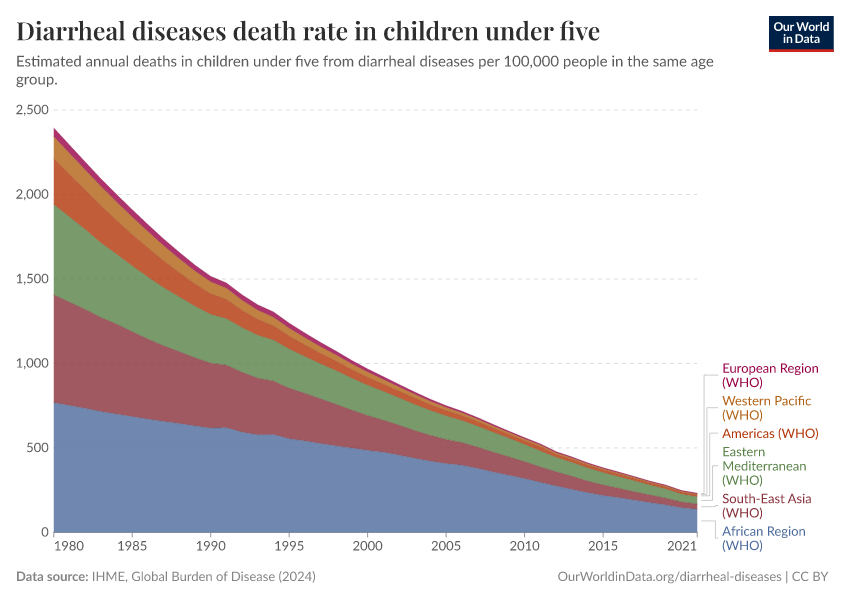
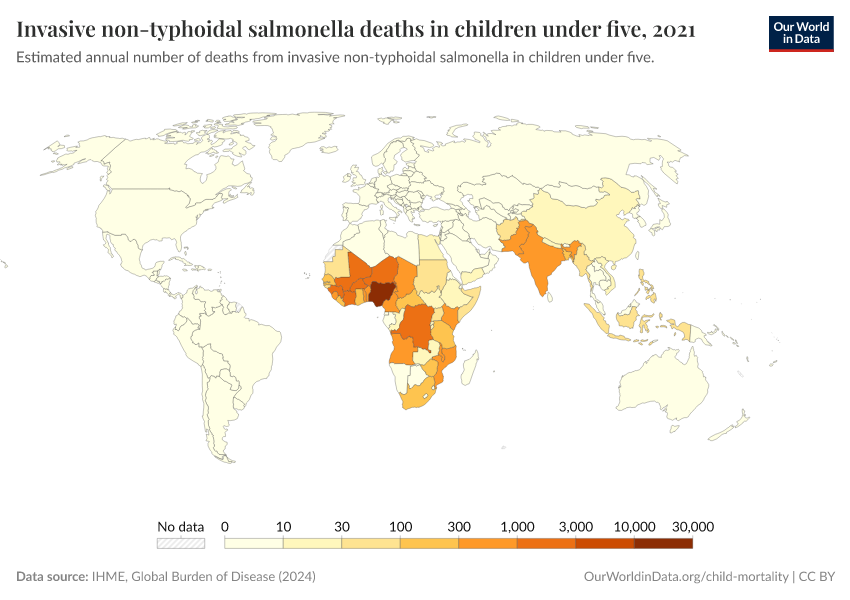
Diarrheal diseases are one of the most common causes of death among children.
It’s estimated that around 340,000 children died from diarrheal diseases globally in 2021. This is shown in the chart, which details the causes of death in children under five.
Deaths from diarrheal diseases have declined over time, but they still carry a substantial death toll today.
This is because people in many countries still lack access to clean water and sanitation, adequate treatment and healthcare, and have low vaccination rates against pathogens that cause diarrheal disease.
What you should know about this data
- These estimates come from the Global Burden of Disease study published by the Institute for Health Metrics (IHME). This is currently one of the few sources that produce global-level estimates across most countries on the prevalence and disease burden of diarrheal diseases.
- Estimates of diarrheal deaths are based on vital registration and verbal autopsy data and a range of hospital and community samples where pathogens were identified using cell culture, immunoassay, and RT-PCR techniques.
- This data was then used to estimate a single underlying cause of death for all deaths in the Global Burden of Disease study.
- There are large differences in the quality and availability of data across the world. While high-quality data in richer countries often exists, data on deaths from diarrheal diseases in many poorer countries is often limited. The IHME Global Burden of Disease attempts to fill these gaps, but these estimates come with a level of uncertainty. This is, therefore, also true for all global figures.

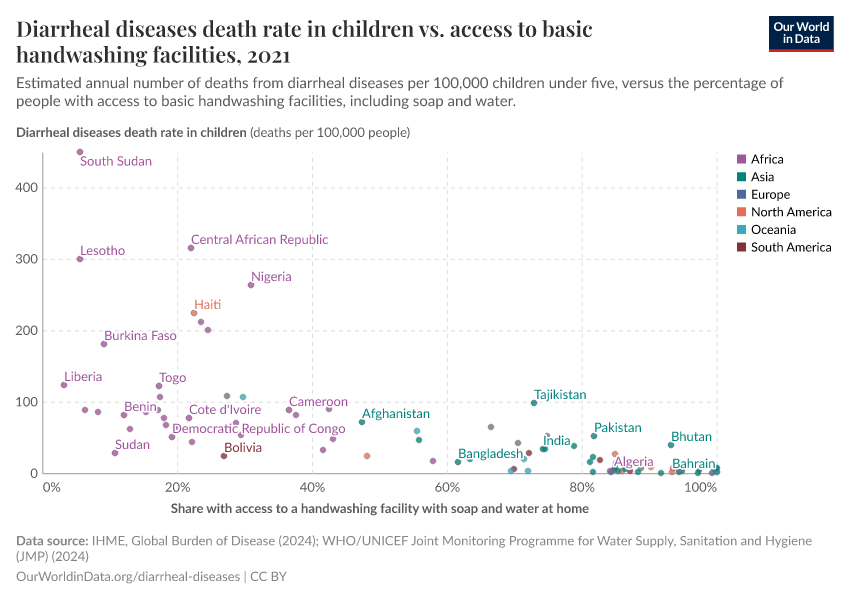
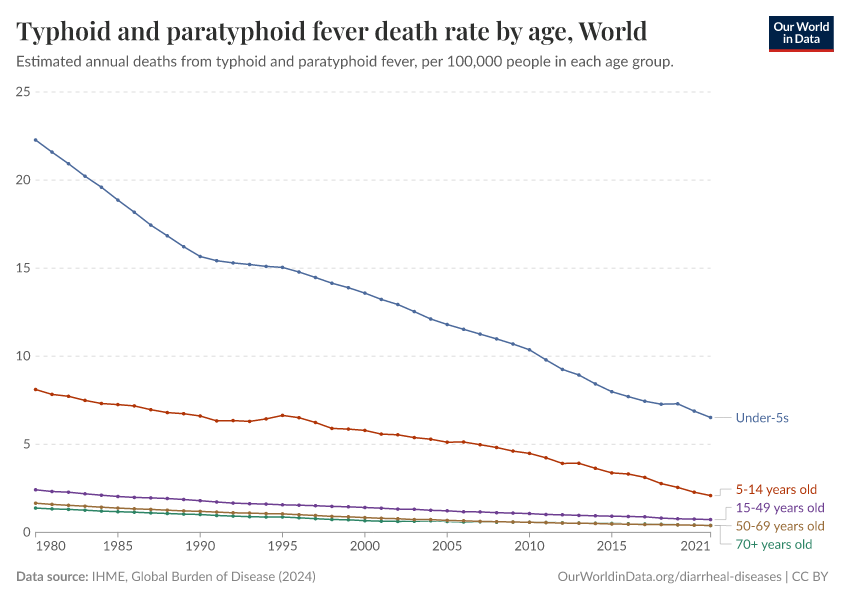
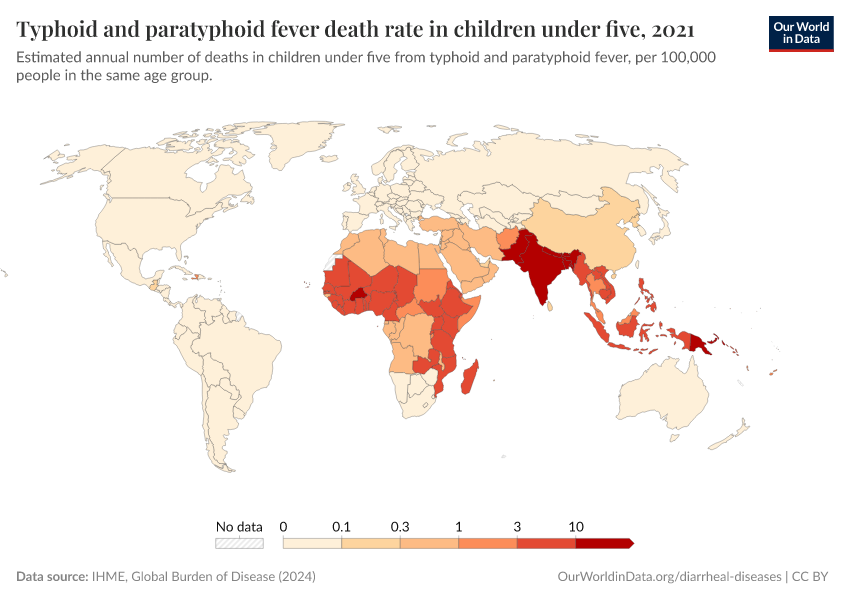
Diarrheal death rates vary widely
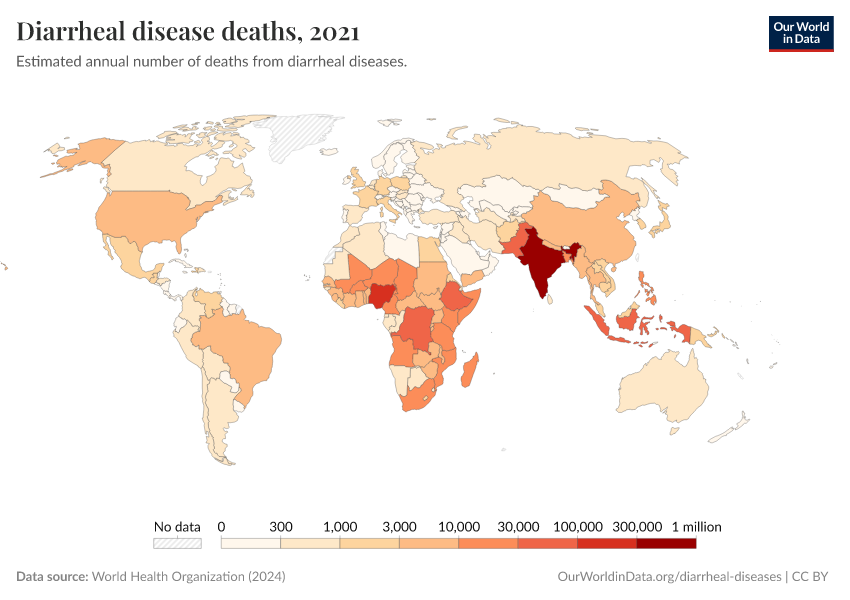
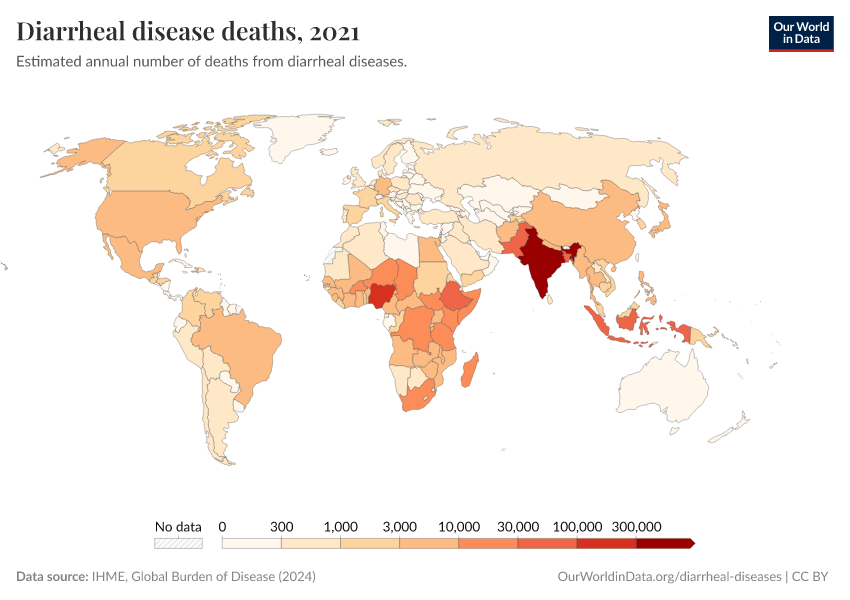
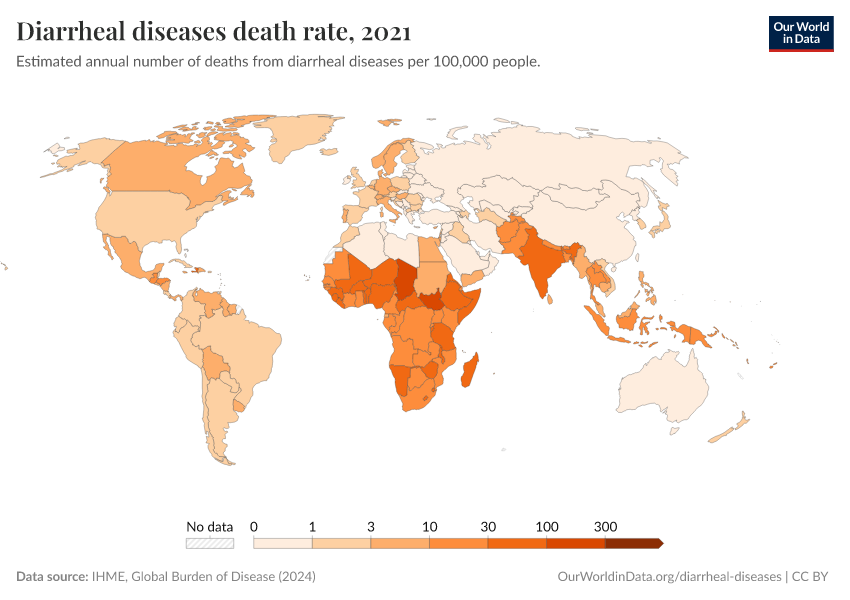
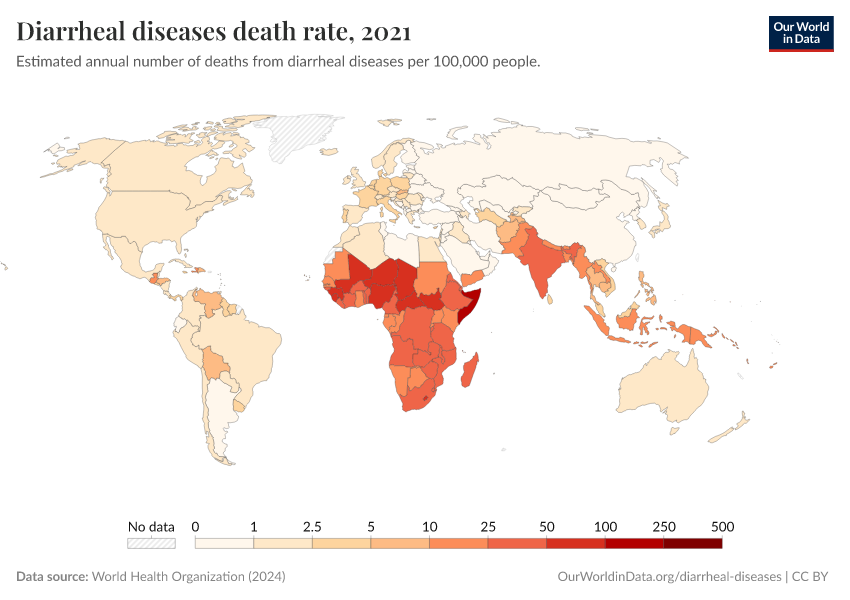
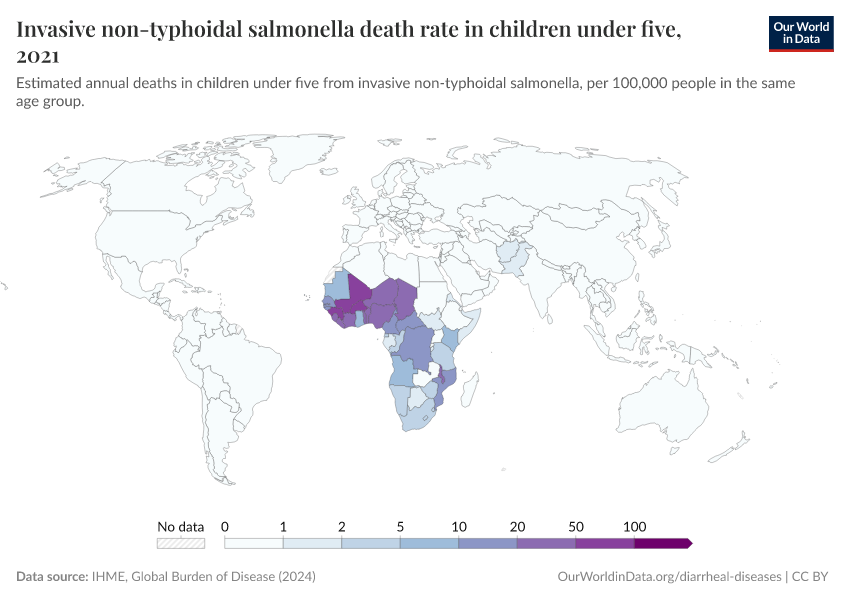
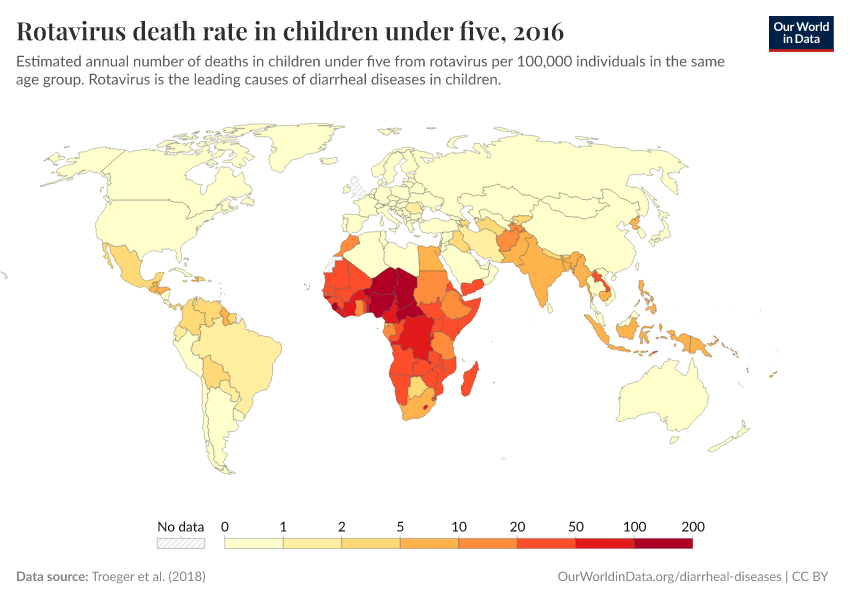
There are significant differences in diarrheal death rates across the world.
This is shown in the map, which reports deaths from diarrheal diseases per 100,000 people.
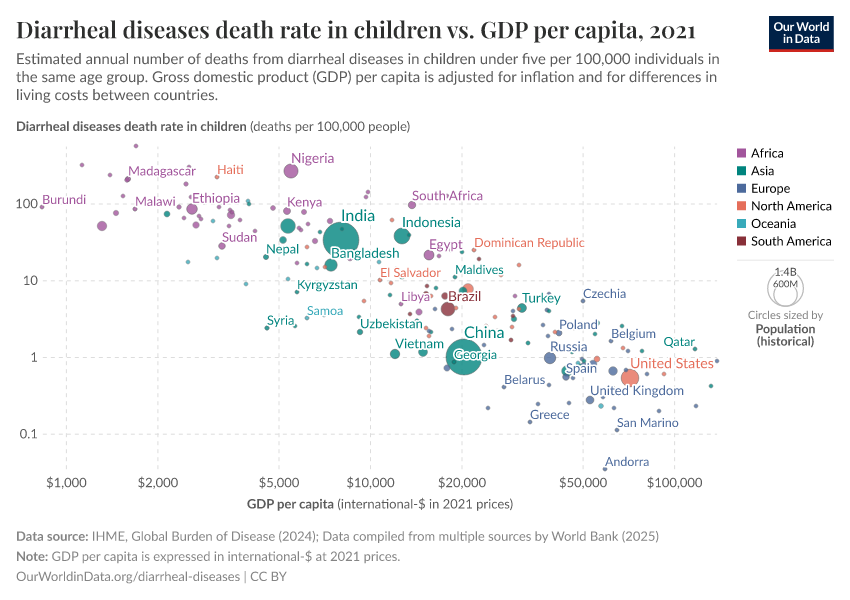
Deaths from diarrheal disease are more common in poorer countries. Death rates in low-income countries are almost fifty times higher than in high-income countries.
Diarrheal deaths remain a large problem in much of the world – even today – but they can be significantly reduced with greater public health efforts.
What you should know about this data
- These estimates come from the Global Burden of Disease study published annually by the Institute for Health Metrics (IHME). This is currently one of the few sources that produces global-level estimates across most countries on the prevalence and disease burden of diarrheal diseases.
- Estimates of diarrheal deaths are based on vital registration and verbal autopsy data and a range of hospital and community samples where pathogens were identified using cell culture, immunoassay, and RT-PCR techniques.
- This data was then used to estimate a single underlying cause of death for all deaths in the Global Burden of Disease study.
- There are large differences in the quality and availability of data across the world. While high-quality data in richer countries often exists, data on deaths from diarrheal diseases in many poorer countries is often limited. The IHME Global Burden of Disease attempts to fill these gaps, but these estimates come with a level of uncertainty. This is therefore also true for all global figures.

Ten pathogens are responsible for most diarrheal deaths in children
Researchers now know that diarrheal disease deaths in children are primarily caused by pathogens, such as viruses, bacteria, and protists.2
The visualization shows the estimated annual number of child deaths globally caused by different viruses, bacteria, and other pathogens. The size of the box is proportional to their share of diarrheal deaths.
Rotavirus is responsible for the greatest share – over one-third – of yearly diarrheal disease deaths in children. It kills over 200,000 children. It is followed by shigella, responsible for more than one in ten.
In total, ten pathogens are responsible for three-quarters of diarrheal deaths.
These pathogens are transmitted between people through different routes, including contaminated water and food, respiratory droplets, and close contact.3
What you should know about this data
- Estimates for the fraction of diarrheal deaths caused by each pathogen come from a study by Adam Cohen et al. (2022).4
- The authors used high-quality data from the Global Pediatric Diarrhea Surveillance (GPDS) network, which included large general hospitals in 28 countries of different income levels. They tested stool samples for various pathogens using molecular techniques and compared these to controls.
- The findings were then extrapolated globally, to estimate the number of deaths worldwide caused by each pathogen, using additional data collected from previous studies, such as the Global Burden of Disease study. There are large differences in the quality and availability of data on diarrheal disease deaths across the world. While high-quality data in richer countries often exists, data on deaths from diarrheal diseases in many poorer countries is often limited. The IHME Global Burden of Disease attempts to fill these gaps, but these estimates come with a level of uncertainty. This is therefore also true for all global figures.
- The share of diarrheal deaths caused by each pathogen can change with public health efforts, such as greater rotavirus vaccination rates and oral rehydration therapy.
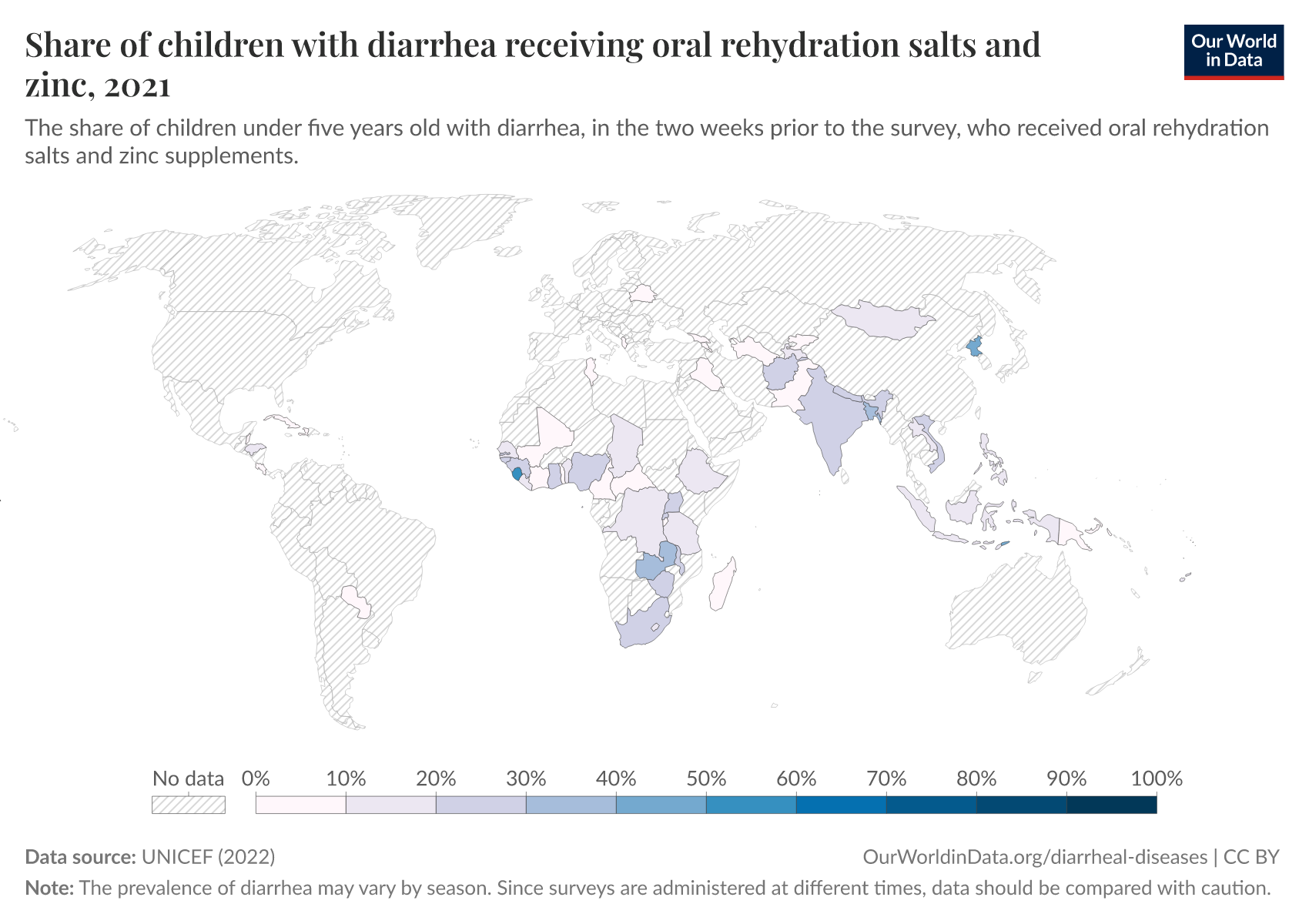
Many children still don’t receive oral rehydration treatment
By understanding the causes of diarrheal diseases, the world has managed to reduce their burden through public health measures.
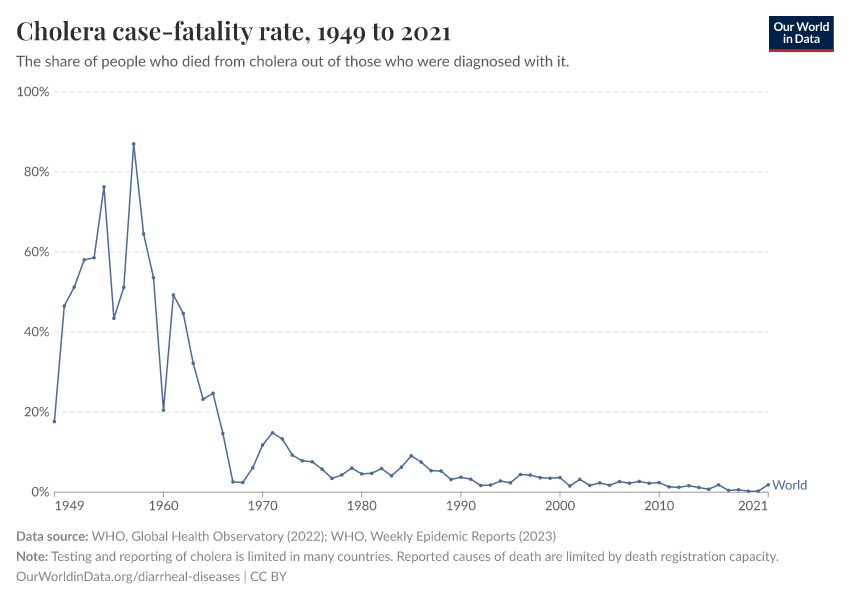
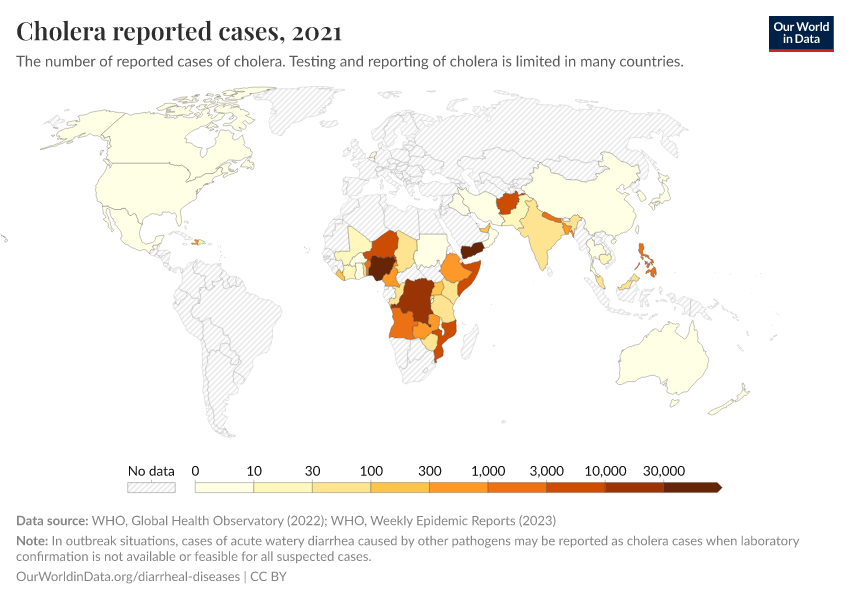
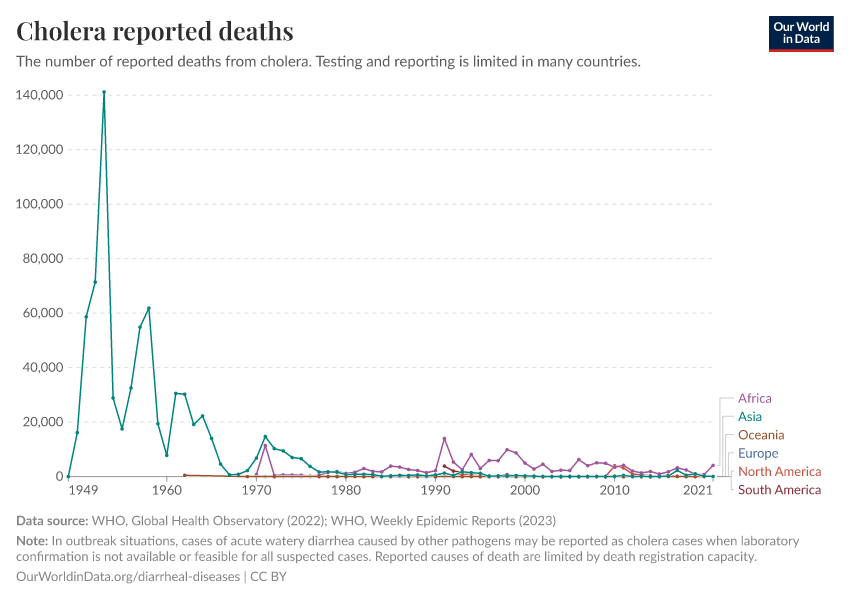
Cholera, for example, used to be far deadlier than it is today. Left untreated, it can cause dehydration and death within hours of the first symptoms.8 During large outbreaks in the 19th century, between 30 and 60% of people diagnosed with cholera then died from it in many major cities, including New York and Berlin.9
This changed when scientists discovered that diarrheal diseases could be treated with a straightforward form of treatment — what patients need is rehydration, using a solution of water, salts, and sugar, which replenish fluids lost, while continuing to feed.
In the 1960s, scientists developed a low-cost version, oral rehydration solution, which can be used easily at home.10
With this understanding, diarrhea can be made much less deadly.11
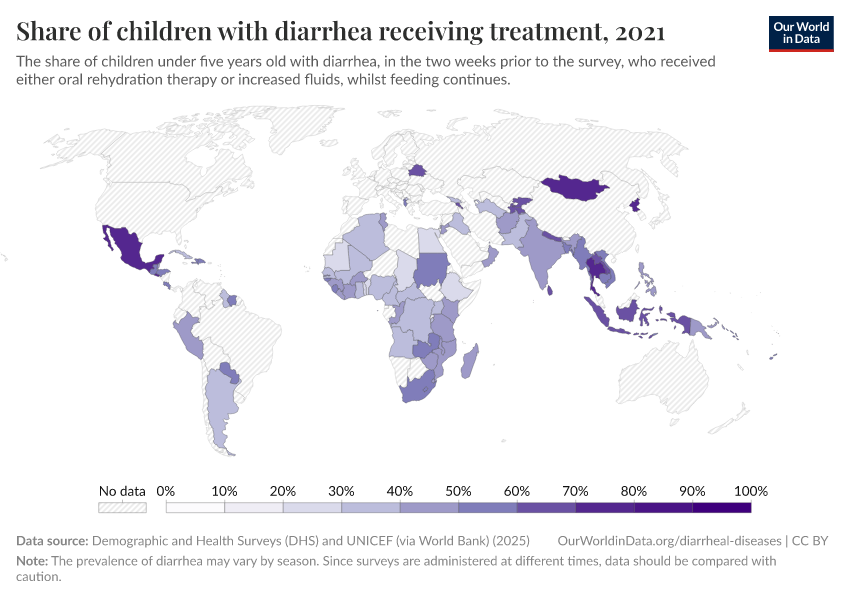
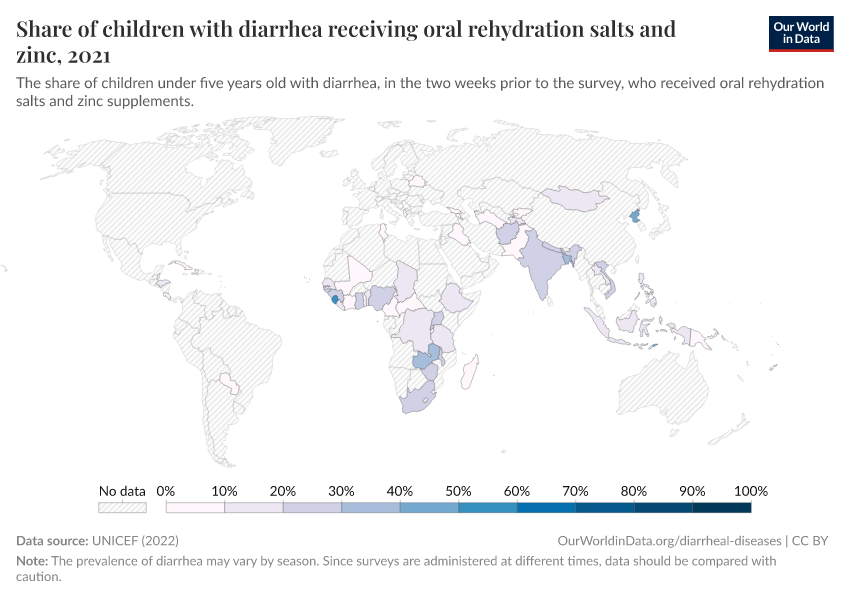
But, in many countries, only a small share of children receive oral rehydration therapy. You can see this in the chart.
This is due to various factors, such as a lack of knowledge about its benefits, limited advocacy and messaging, and low treatment supply.12
By providing more children with treatment, the burden of diarrheal diseases can be reduced significantly.
What you should know about this data
- Oral rehydration therapy is effective at replacing fluid loss in many diarrheal diseases.
- Additional medications, such as antibiotics and antiparasitic treatments, may also be needed to treat some diarrheal diseases.

Rotavirus vaccination can prevent around a hundred thousand deaths each year
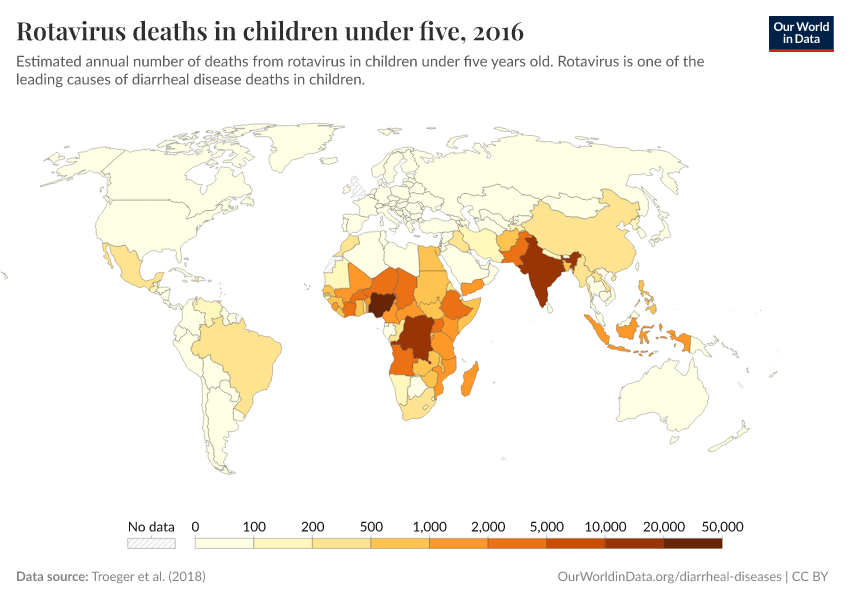
Rotavirus is the most common cause of diarrheal deaths in children globally.
Although rotavirus vaccines were first introduced in the United States in 2006, the death rate remains high because children in many countries do not receive vaccinations.
In addition, the efficacy of rotavirus vaccines has been lower in countries with higher mortality rates.13
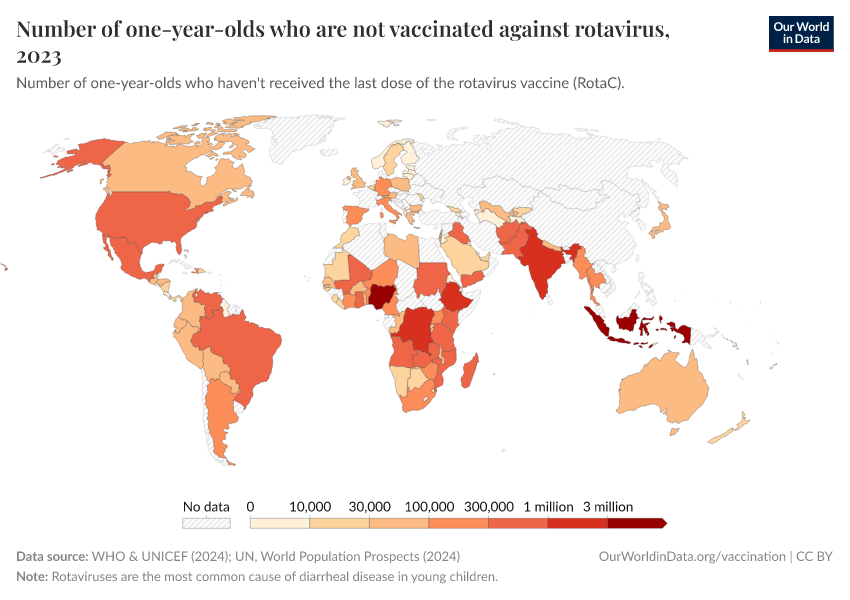
In the chart, you can see the share of one-year-olds who were vaccinated against rotavirus.
Vaccination rates were high in some countries, such as Ghana, Kenya, and Tajikistan, with rates above 90% in 2021. But in other countries, they were much lower: for example, fewer than 1-in-5 children in Congo were vaccinated.
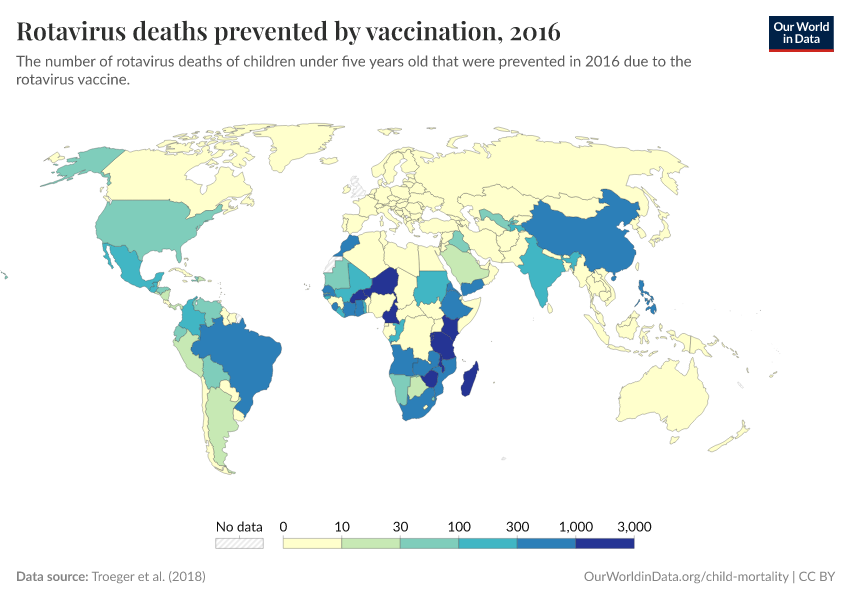
By increasing vaccination rates, more children can be protected against the virus, and a major cause of diarrheal deaths can be prevented.14
What you should know about this data
- Rotavirus vaccines are typically given in several doses, typically two or three, depending on the vaccine.
- This shows the share of one-year-olds who had received the final dose.

Research & Writing
August 16, 2019
More than half a million children die from diarrhea each year. How do we prevent this?
Despite being treatable and preventable, 1.6 million people died from diarrheal diseases in 2017; one-third were children under five years old. This makes it one of the largest killers of children. Here we look at where and why children are dying from diarrheal diseases, and what we can do to stop this.
August 22, 2019
Rotavirus vaccine - an effective tool that prevents children dying from diarrhea
Rotavirus is the leading cause of diarrheal deaths in children. There is, however, an effective tool against it: the rotavirus vaccine.
More articles on Diarrheal Diseases
Key Charts on Diarrheal Diseases
See all charts on this topic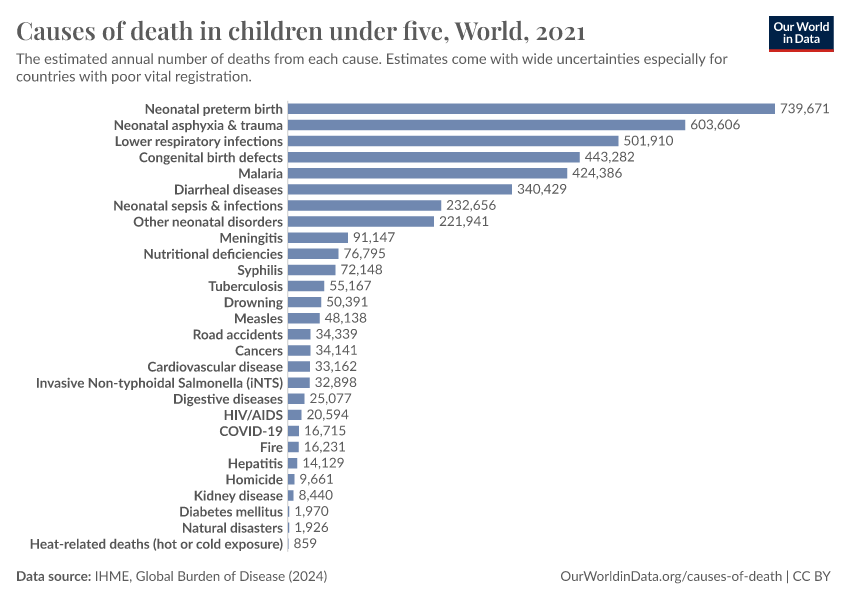









































Featured Data on Diarrheal Diseases
Endnotes
It’s estimated that 1.17 million people died from diarrheal diseases in 2021. Meanwhile, it’s estimated that around 746,000 died from suicide, around 397,000 died from homicide, and around 96,500 died in conflict and terrorism that year; these add up to 1.24 million. These estimates come from the IHME’s Global Burden of Disease study, and you can explore the data here.
Protists are single-celled organisms that don’t fit into other categories, such as fungi, animals, or plants.
Webb, C., & Cabada, M. M. (2018). A Review on Prevention Interventions to Decrease Diarrheal Diseases’ Burden in Children. Current Tropical Medicine Reports, 5(1), 31–40. https://doi.org/10.1007/s40475-018-0134-x
Cohen, A. L., Platts-Mills, J. A., Nakamura, T., Operario, D. J., Antoni, S., Mwenda, J. M., Weldegebriel, G., Rey-Benito, G., De Oliveira, L. H., Ortiz, C., Daniels, D. S., Videbaek, D., Singh, S., Njambe, E., Sharifuzzaman, M., Grabovac, V., Nyambat, B., Logronio, J., Armah, G., … Serhan, F. (2022). Aetiology and incidence of diarrhoea requiring hospitalisation in children under 5 years of age in 28 low-income and middle-income countries: Findings from the Global Pediatric Diarrhea Surveillance network. BMJ Global Health, 7(9), e009548. https://doi.org/10.1136/bmjgh-2022-009548
Deaths from cholera were primarily found in South Asia in this study.
Kremer, M., Luby, S. P., Maertens, R., Tan, B., & Więcek, W. (2023). Water Treatment And Child Mortality: A Meta-Analysis And Cost-effectiveness Analysis (No. w30835). National Bureau of Economic Research. Available here.
Santosham, M., Duggan, C. P., & Glass, R. (2019). Elimination of diarrheal mortality in children – the last half million. Journal of Global Health, 9(2), 020102. https://doi.org/10.7189/jogh.09.020102
Alsan, M., & Goldin, C. (2019). Watersheds in child mortality: The role of effective water and sewerage infrastructure, 1880–1920. Journal of Political Economy, 127(2), 586-638
Guerrant, R. L., Carneiro-Filho, B. A., & Dillingham, R. A. (2003). Cholera, Diarrhea, and Oral Rehydration Therapy: Triumph and Indictment. Clinical Infectious Diseases, 37(3), 398–405. https://doi.org/10.1086/376619
Cutler, D., & Miller, G. (2005). The role of public health improvements in health advances: The twentieth-century United States. Demography, 42(1), 1–22. https://doi.org/10.1353/dem.2005.0002
Van Poppel, F., & Van der Heijden, C. (1997). The effects of water supply on infant and childhood mortality: A review of historical evidence. Health Transition Review, 113–148. https://ocw.tudelft.nl/wp-content/uploads/Childhood-Mortality.pdf
Shulman, S. T. (2004). The History of Pediatric Infectious Diseases. Pediatric Research, 55(1), 163–176. https://doi.org/10.1203/01.PDR.0000101756.93542.09
These figures are the death rates among children under 2 years old.
Burström, B., Macassa, G., Öberg, L., Bernhardt, E., & Smedman, L. (2005). Equitable child health interventions: The impact of improved water and sanitation on inequalities in child mortality in Stockholm, 1878 to 1925. American Journal of Public Health, 95(2), 208–216. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1449154/
Macassa, G., Ponce de Leon, A., & Burström, B. (2006). The impact of water supply and sanitation on area differentials in the decline of diarrhoeal disease mortality among infants in Stockholm 1878—1925. Scandinavian Journal of Public Health, 34(5), 526–533. https://ajph.aphapublications.org/doi/pdf/10.2105/AJPH.2003.034900
Helgertz, J., & Önnerfors, M. (2019). Public water and sewerage investments and the urban mortality decline in Sweden 1875–1930. The History of the Family, 24(2), 307–338. https://doi.org/10.1080/1081602X.2018.1558411
Harris, J. B., LaRocque, R. C., Qadri, F., Ryan, E. T., & Calderwood, S. B. (2012). Cholera. The Lancet, 379(9835), 2466–2476. https://doi.org/10.1016/S0140-6736(12)60436-X
Chan, C. H., Tuite, A. R., & Fisman, D. N. (2013). Historical Epidemiology of the Second Cholera Pandemic: Relevance to Present Day Disease Dynamics. PLoS ONE, 8(8), e72498. https://doi.org/10.1371/journal.pone.0072498
Oral rehydration solution effectively replaces fluid loss in many diarrheal diseases, not just cholera.
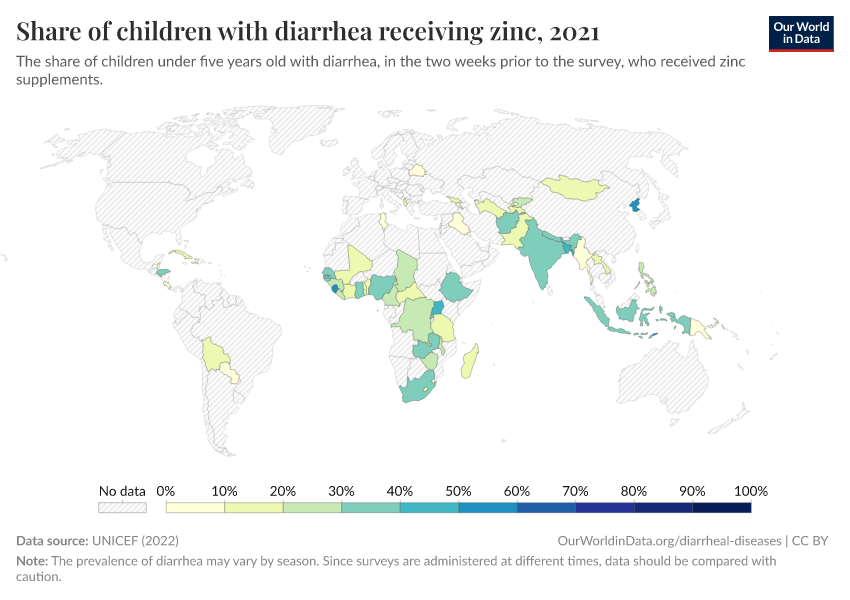
Zinc supplementation also reduces diarrheal diseases and can be provided with oral rehydration solution.
Additional medications, such as antibiotics and antiparasitic treatments, may also be needed to treat some diarrheal diseases.
Zinc Supplementation in Acute Diarrhea is Acceptable, Does Not Interfere with Oral Rehydration, and Reduces the Use of Other Medications: A Randomized Trial in Five Countries. (2006). Journal of Pediatric Gastroenterology & Nutrition, 42(3), 300–305. https://doi.org/10.1097/01.mpg.0000189340.00516.30
Santosham, M., Chandran, A., Fitzwater, S., Fischer-Walker, C., Baqui, A. H., & Black, R. (2010). Progress and barriers for the control of diarrhoeal disease. The Lancet, 376(9734), 63–67. https://doi.org/10.1016/S0140-6736(10)60356-X
Black, R. E. (2019). Progress in the use of ORS and zinc for the treatment of childhood diarrhea. Journal of Global Health, 9(1), 010101. https://doi.org/10.7189/jogh.09.010101
Patel, A., Mamtani, M., Dibley, M. J., Badhoniya, N., & Kulkarni, H. (2010). Therapeutic Value of Zinc Supplementation in Acute and Persistent Diarrhea: A Systematic Review. PLoS ONE, 5(4), e10386. https://doi.org/10.1371/journal.pone.0010386
Kanungo, S., Azman, A. S., Ramamurthy, T., Deen, J., & Dutta, S. (2022). Cholera. The Lancet, 399(10333), 1429–1440. https://doi.org/10.1016/S0140-6736(22)00330-0
Deen, J., Mengel, M. A., & Clemens, J. D. (2020). Epidemiology of cholera. Vaccine, 38, A31–A40. https://doi.org/10.1016/j.vaccine.2019.07.078
Santosham, M., Duggan, C. P., & Glass, R. (2019). Elimination of diarrheal mortality in children – the last half million. Journal of Global Health, 9(2), 020102. https://doi.org/10.7189/jogh.09.020102
Bhattacharya, S. K. (1994). History of development of oral rehydration therapy. Indian Journal of Public Health, 38(2), 39–43. https://pubmed.ncbi.nlm.nih.gov/7530695/
Binder, H. J., Brown, I., Ramakrishna, B. S., & Young, G. P. (2014). Oral Rehydration Therapy in the Second Decade of the Twenty-first Century. Current Gastroenterology Reports, 16(3), 376. https://doi.org/10.1007/s11894-014-0376-2
The case-fatality rate of cholera now ranges between 0 to 10% globally. However, this figure has limitations: many countries lack surveillance and reporting of cholera cases. Furthermore, some countries use different definitions of cases due to a lack of testing capacity. For example, some countries describe all cases of watery diarrhea as cholera cases during outbreaks due to limited laboratory capacity.
The case-fatality rate has also risen during large outbreaks from conflict and natural disasters, when people may lack access to clean water, sanitation, and treatments.
Ganesan, D., Gupta, S. S., & Legros, D. (2020). Cholera surveillance and estimation of burden of cholera. Vaccine, 38, A13–A17. https://doi.org/10.1016/j.vaccine.2019.07.036
Wiens, K. E., Xu, H., Zou, K., Mwaba, J., Lessler, J., Malembaka, E. B., Demby, M. N., Bwire, G., Qadri, F., Lee, E. C., & Azman, A. S. (2022). Towards estimating true cholera burden: A systematic review and meta-analysis of Vibrio cholerae positivity [Preprint]. MedRxiv. https://doi.org/10.1101/2022.10.05.22280736
Ezezika, O., Ragunathan, A., El-Bakri, Y., & Barrett, K. (2021). Barriers and facilitators to implementation of oral rehydration therapy in low- and middle-income countries: A systematic review. PLOS ONE, 16(4), e0249638. https://doi.org/10.1371/journal.pone.0249638
Santosham, M., Chandran, A., Fitzwater, S., Fischer-Walker, C., Baqui, A. H., & Black, R. (2010). Progress and barriers for the control of diarrhoeal disease. The Lancet, 376(9734), 63–67. https://doi.org/10.1016/S0140-6736(10)60356-X
The effectiveness of rotavirus vaccines has been around 86% among children under 12 months in countries with low rotavirus mortality, and 63 or 66% in countries with high rotavirus mortality.
Burnett, E., Parashar, U. D., & Tate, J. E. (2020). Real-world effectiveness of rotavirus vaccines, 2006–19: A literature review and meta-analysis. The Lancet Global Health, 8(9), e1195–e1202. https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(20)30262-X/fulltext
The reasons for a lower efficacy in poorer countries are unknown but may result from many factors. For example, other oral vaccines, including vaccines against polio and cholera, have also shown lower efficacies in poorer countries. This may be because children have co-infections with other enteric viruses, which reduce their gut immune response to the vaccines. Other potential factors include higher exposure to the virus and variations in gut microbiomes, blood groups, and immune antigens.
Burke, R. M., Tate, J. E., Kirkwood, C. D., Steele, A. D., & Parashar, U. D. (2019). Current and new rotavirus vaccines: Current Opinion in Infectious Diseases, 32(5), 435–444. https://doi.org/10.1097/QCO.0000000000000572
Burnett, E., Parashar, U., & Tate, J. (2018). Rotavirus Vaccines: Effectiveness, Safety, and Future Directions. Pediatric Drugs, 20(3), 223–233. https://doi.org/10.1007/s40272-018-0283-3
Kirkwood, C. D., Ma, L.-F., Carey, M. E., & Steele, A. D. (2019). The rotavirus vaccine development pipeline. Vaccine, 37(50), 7328–7335. https://doi.org/10.1016/j.vaccine.2017.03.076
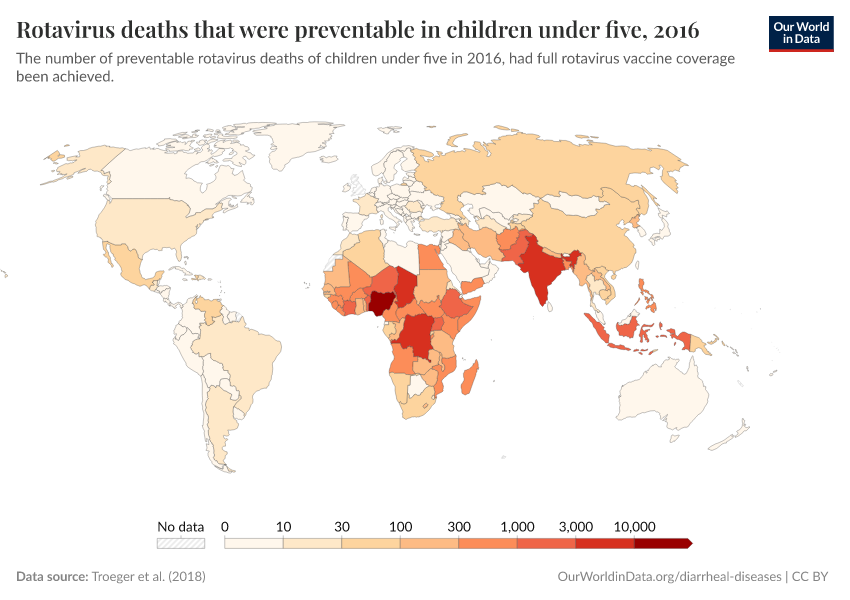
Troeger, C., Khalil, I. A., Rao, P. C., Cao, S., Blacker, B. F., Ahmed, T., Armah, G., Bines, J. E., Brewer, T. G., Colombara, D. V., Kang, G., Kirkpatrick, B. D., Kirkwood, C. D., Mwenda, J. M., Parashar, U. D., Petri, W. A., Riddle, M. S., Steele, A. D., Thompson, R. L., … Reiner, R. C. (2018). Rotavirus Vaccination and the Global Burden of Rotavirus Diarrhea Among Children Younger Than 5 Years. JAMA Pediatrics, 172(10), 958. https://doi.org/10.1001/jamapediatrics.2018.1960
The authors estimate that the rotavirus averted around 28,000 deaths in children under five in 2016. They also estimate that an additional 83,200 deaths in this age group could have been averted if full vaccine coverage had been achieved that year.
Cite this work
Our articles and data visualizations rely on work from many different people and organizations. When citing this topic page, please also cite the underlying data sources. This topic page can be cited as:
Saloni Dattani, Fiona Spooner, Hannah Ritchie, and Max Roser (2023) - “Diarrheal Diseases” Published online at OurWorldinData.org. Retrieved from: 'https://ourworldindata.org/diarrheal-diseases' [Online Resource]BibTeX citation
@article{owid-diarrheal-diseases,
author = {Saloni Dattani and Fiona Spooner and Hannah Ritchie and Max Roser},
title = {Diarrheal Diseases},
journal = {Our World in Data},
year = {2023},
note = {https://ourworldindata.org/diarrheal-diseases}
}Reuse this work freely
All visualizations, data, and articles produced by Our World in Data are completely open access under the Creative Commons BY license. You have the permission to use, distribute, and reproduce these in any medium, provided the source and authors are credited.
The data produced by third parties and made available by Our World in Data is subject to the license terms from the original third-party authors. We will always indicate the original source of the data in our documentation, so you should always check the license of any such third-party data before use and redistribution.
All of our charts can be embedded in any site.