Maternal Mortality
This page was first published in November 2013, and we updated the text in February 2024.
What could be more tragic than a mother losing her life while she is pregnant or giving birth to a baby?
On this page, we present global data and research on maternal mortality — pregnancy-related death — how it varies around the world, how much it has been reduced over time, and what we can do to reduce the risk of pregnancy-related death further.
See all interactive charts on maternal mortality ↓
Related topics:
Other research and writing on maternal mortality on Our World in Data:
Maternal mortality: What does it mean?
The World Health Organization (WHO) estimates that around 300,000 women globally died from pregnancy-related deaths in 2017, which is around 800 each day on average.
According to the ICD-11, maternal deaths are defined as the deaths of women while pregnant or within 42 days of termination of pregnancy, from pregnancy-related causes, but excluding accidental or incidental causes of death.
In the WHO Mortality Database and IHME GBD (estimates up to 2019), maternal deaths up to 1 year of termination of pregnancy are also included.1
Two additional indicators of maternal mortality are commonly used:
- Maternal Mortality Rate — which refers to the number of pregnancy-related deaths in a year divided by the number of women of reproductive age (normally 15 to 49 years old) alive that year
- Maternal Mortality Ratio — which is a ratio comparing the number of pregnancy-related deaths to the number of births in the same period
How do pregnancy-related deaths vary globally?
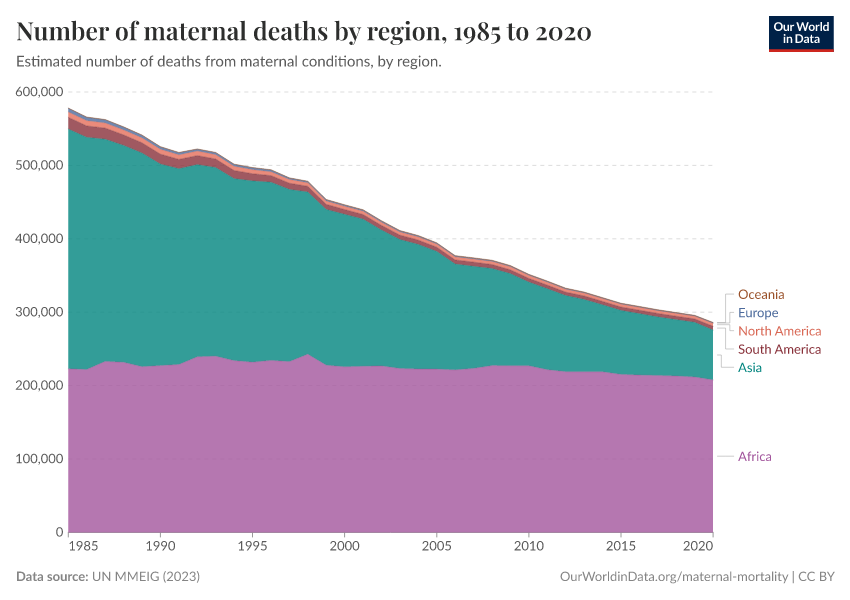
In the chart here, we see global pregnancy-related deaths by region. Most occurred in Sub-Saharan Africa, and a sizeable share occurred in South Asia.
This is partly because many more babies are born in Asia and Africa than in other regions.
But a more important factor is the much higher maternal mortality rates found in lower-income countries, as we’ll see below.

In the map, we see the annual number of pregnancy-related deaths by country. Again, this is a reflection of both the number of births each year and the risk that a mother will die as a result.

Where are women most at risk of dying in childbirth?
Where are women most at risk of dying from pregnancy-related causes today?
Here two indicators are important. First, the risk per pregnancy. Second, the lifetime risk to a woman, which also depends on the number of children she has.
Risk of death per birth
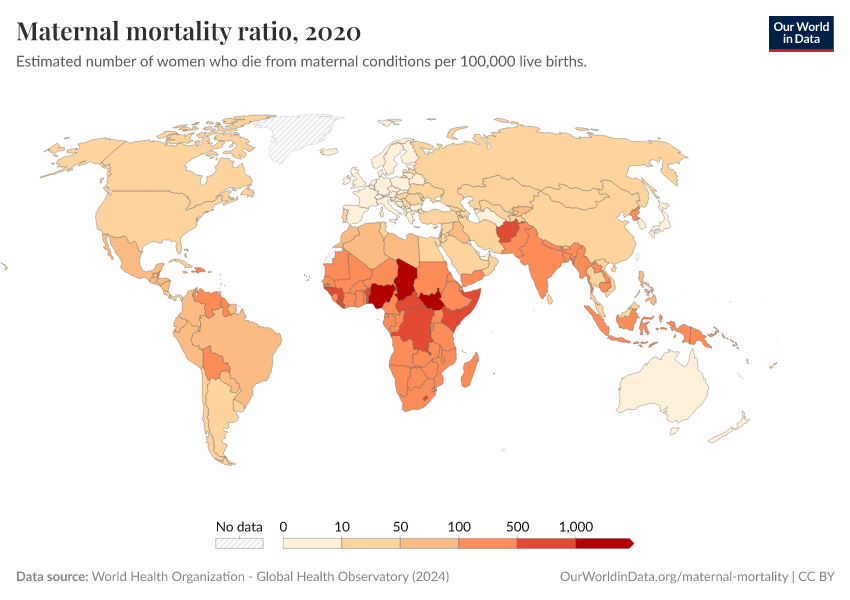
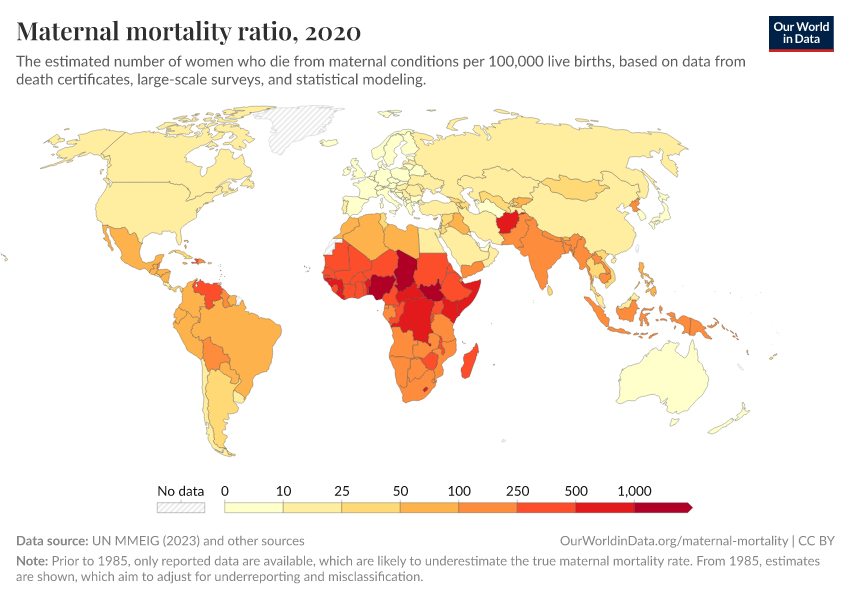
In the chart below we see the maternal mortality ratio across the world.
What becomes clear from the map scale — spanning orders of magnitude — is the extent of cross-country inequality: the magnitude of the differences in mortality between countries are very large.
In high-income countries, the maternal mortality ratio was around 11 per 100,000 live births in 2017. But in low-income countries, it was around 450 per 100,000 — around 40 times higher.
Maternal mortality tends to be especially high in sub-Saharan Africa, South America, and South and South-East Asia.

Lifetime risk of death from pregnancy-related causes
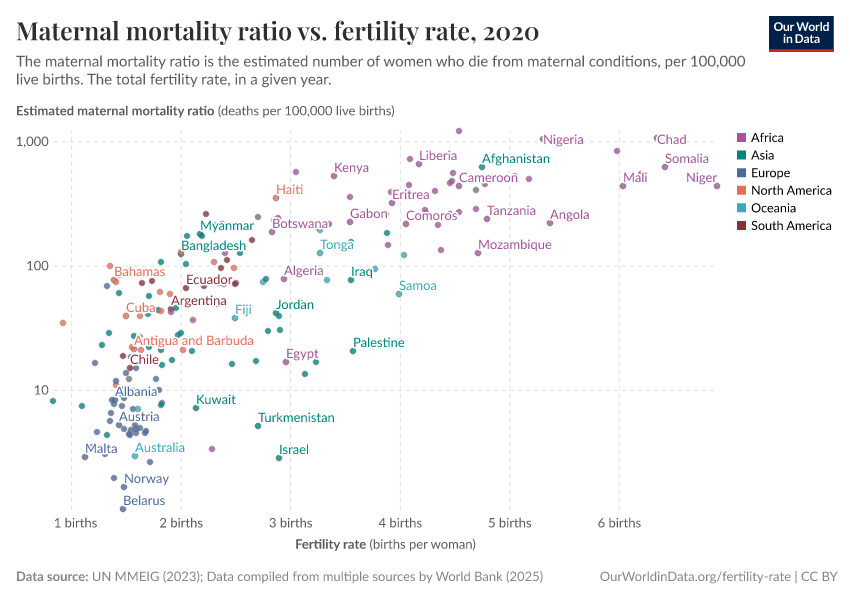
Of course, the chances that a woman dies from maternal causes are not only dependent on the risk per pregnancy — which we looked at above — but also the number of pregnancies she has.
Maternal mortality is higher in poorer regions, and the overall risks tend to be higher where women have more children. These amplify the differences in risk between high and low-income countries.
In the chart, we see estimates of the share of women who would die from maternal causes in their lifetime.
This is based on a period measure — using current maternal mortality and fertility rates — and assumes that the rates of mortality and fertility seen at different ages today are equal to the rates that women will experience throughout their lifespans.
Across most of the world, the risk is less than 1%. In fact, in most countries, it’s even well below 0.1%.
But, in countries in sub-Saharan Africa, South America, and South and South-East Asia, the risk is much higher.

What we know is possible
Maternal mortality can be reduced substantially
A large number of pregnancy-related deaths can be avoided. The visualization below shows this using three scenarios:
- How many mothers would die today if we still had the very poor health of the past? Even the countries with the best maternal health today used to have very high maternal mortality rates in the past. In Sweden and Finland in 1800, for example, around 900 mothers died for every 100,000 live births, nearly one in a hundred.2 In a world where 140 million women give birth each year this would mean that 1.26 million would die.
- The world in 2015: the actual number of women who died from pregnancy-related causes in 2015 was 302,700.
- If all regions had the health of the best-off countries: In 2015, the world region with the lowest maternal mortality was the European Union, where 8 women died per 100,000 live births. In the world of 2015, where 140 million women give birth each year, if all countries had this level of maternal mortality, far fewer — 11,000 — would die.3
We can see how much global maternal health has improved, but we can also see how much further we could go.
If all regions achieved the healthcare and living standards of the EU, there would be almost 300,000 fewer deaths, a reduction of over 95%.
If we think of it in this way, almost all of the world’s pregnancy-related deaths are preventable with improvements in adequate maternal care, safe deliveries, good nutrition and hygiene and sanitation.4
Read more in our article:
How has maternal mortality changed over the long term?
Risks and health complications from childbirth have been tragic but not uncommon for mothers throughout history.
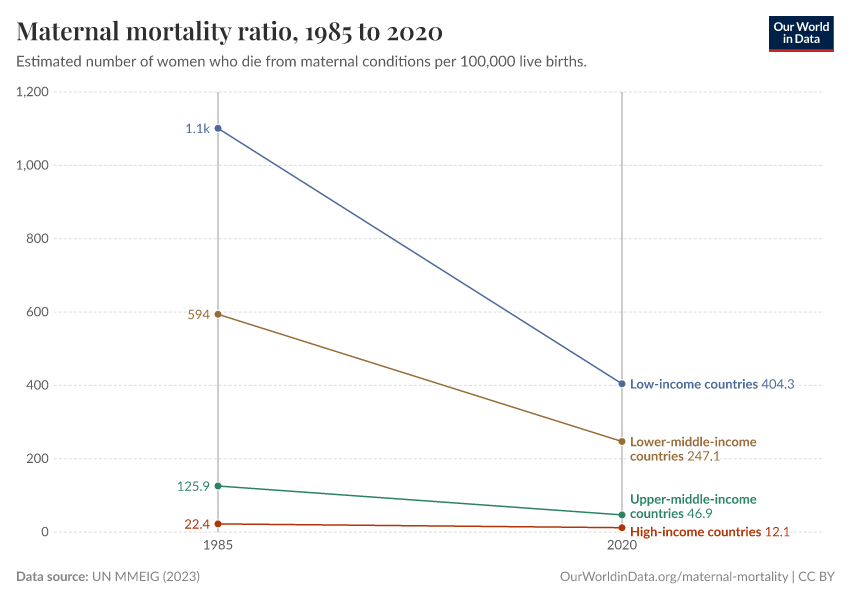
The decline in maternal mortality over the last generations is shown in the chart. We see that in some countries in the 19th century, around 500 to 1,000 mothers died per 100,000 births, which is between 1 in 100 and 1 in 200.
Since women tended to have more children in the past, pregnancy-related death was not uncommon.
This changed over the last century and today most rich countries have a maternal mortality ratio below 10 deaths per 100,000 births, which is a decline of between 50- to 100-fold.

The dramatic decline in maternal mortality is due to improvements in understanding the causes of maternal mortality and the adoption of practices to prevent it.
For example, in the 20th century, the availability of antibiotics made it possible to treat cases of puerperal fever, and the death of a mother from this condition is today much less common.
As is often the case, we can also see that it takes much less time for countries to catch up to a given standard than other pioneering countries have in the past.
The decline of maternal mortality in Finland, for example, began in the middle of the 19th century and didn’t reach today’s low level more than a century later. In contrast, India and Afghanistan, for example, have achieved large declines much later, but in a shorter amount of time.
Decline of maternal mortality across the world
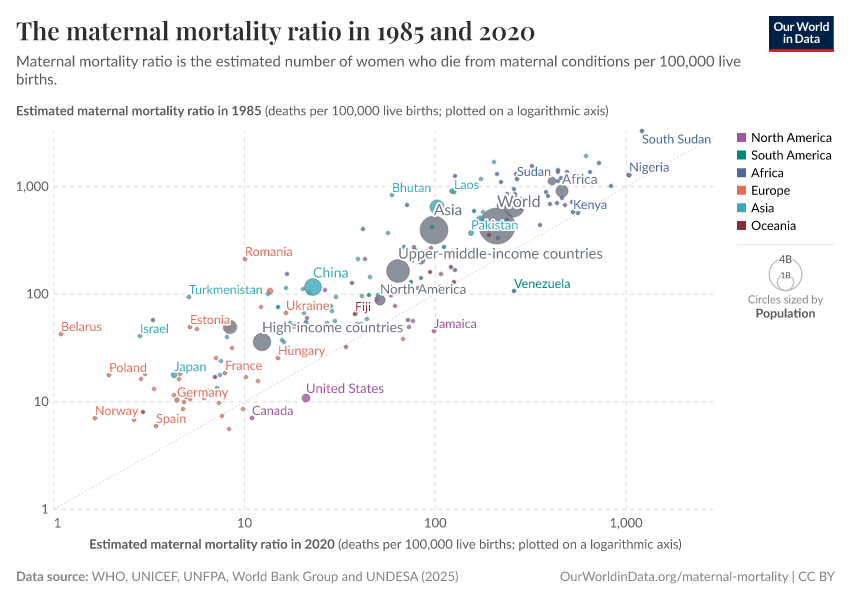
In the majority of countries maternal mortality has declined
Maternal mortality has fallen globally, and for some countries, there has been a dramatic decline. But is this true for all countries? Is maternal mortality falling everywhere?
The chart here compares the maternal mortality ratio in 1990 and later, in 2017.
The grey line shows where countries would fall in which the rate remained unchanged. Here we see that almost all countries lie above this line: that is, the maternal mortality rate in 1990 was higher than in 2017, meaning that the maternal mortality rate has fallen since then.

How do we reduce maternal mortality?
Basic hygiene — the lifesaving discovery of Ignaz Semmelweis
The story of the decline of maternal mortality is about scientific research and the importance of measurement. Today, medicine makes progress by relying on randomized controlled trials — and the history of the decline of maternal mortality started with a kind of controlled trial, one that wasn't planned, but which happened almost accidentally.
In the mid-19th century, the largest maternity hospital in the world was in Vienna. At the time, puerperal sepsis was the most common cause of death in pregnancy. The infection of the uterus killed new mothers shortly after childbirth.5
The Vienna Maternity Hospital was divided into two wings and, for some time, the doctors had noticed a stark difference between the wings that they were not able to explain.
Doctors and medical students were taught in the first wing, while midwives were taught in the second. In the first wing, every tenth (!) mother died of puerperal sepsis, while in the second, "only” one in 25 died.
Crucially, women were admitted to the clinics not based on how complicated their pregnancy was, but simply on alternate days — in other words, by an almost random allocation. Unintentionally, the hospital had created the conditions suitable for a natural experiment.
In 1846, the young Viennese doctor Ignaz Semmelweis was appointed to the hospital. He had the suspicion that the differences in the routine practices of the two wings would give him insight into what was causing the alarmingly high mortality rates in one.
He noticed that in the first wing, where 10% of young mothers perished, medical students alternated between helping women to give birth and attending post-mortem examinations of women who had died of puerperal sepsis. They carried out their work in ordinary daytime clothing rather than clean, white coats, and between autopsies and deliveries, they did not wash their hands.
By contrast, the pupil midwives in the second clinic did not perform postmortem examinations. Thus, many years before germ theory had been developed, Semmelweis concluded that the disease was contagious and that it was the doctors who were transmitting it.
Semmelweis also found that a chemical would destroy the agent that led to the disease, and therefore insisted that his students disinfect their hands with it before attending the pregnancy wards.
This led to dramatic results. By 1848, the maternal mortality rates of the two clinics in the Vienna Maternity Hospital were comparable.6
However, Semmelweis's insistence on his discovery that puerperal sepsis was contagious did not fit into the accepted medical understanding of the time, and this meant an agonizingly slow process of convincing the medical establishment of the importance of better hygiene and measures of antisepsis.
Only in the second half of the 19th century was antisepsis widely introduced into routine obstetric practice. But this change — coupled with the discovery of antibiotics and the development of blood transfusion in the first half of the 20th century — sharply drove down the risk of dying in childbirth.
Semmelweis's story tells us two things.
First, it shows how powerful measurement can be. Decades before the modern germ theory of disease was accepted, and with no understanding of the mechanism that caused puerperal sepsis, it was the measurement of the distribution of pregnancy-related deaths that gave Semmelweis the crucial insight into what steps could be taken to reduce maternal mortality effectively.
Second, it tells us how frustratingly long it can take until discoveries become accepted and finally change practices. Semmelweis's discovery, which could have led to immediate and widespread improvements, was not widely circulated. More time would have to pass, with more knowledge accumulated, before steep reductions in maternal mortality could take place.
We collaborated with the team from Kurz Gesagt and the Bill and Melinda Gates Foundation to tell this history of maternal mortality in a video for the Goalkeepers event in 2017:
What share of births are attended by health staff?
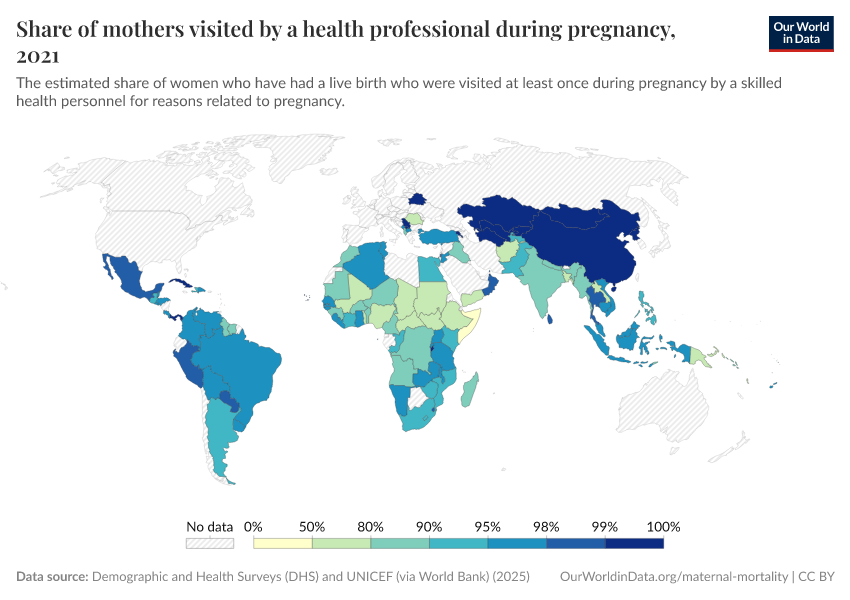
An important factor in a safe delivery for both the mother and baby is receiving good advice, care, and supervision by trained medical staff. But not all births are attended by trained medical personnel.
In the first chart, you can see the share of births that are attended by skilled health staff. For most countries this is close to 100%. But there are still some countries where healthcare access is much lower.
In the second chart, we see the relationship between the maternal mortality rate and the share of births which are attended by skilled health staff.
There is a cluster in the bottom-right corner: this shows countries where the maternal mortality rate is low, and almost all births are attended by skilled personnel.
But we also see countries with much lower staff coverage towards the left. For countries where health staff coverage was lower, we see that typically maternal mortality was much higher.


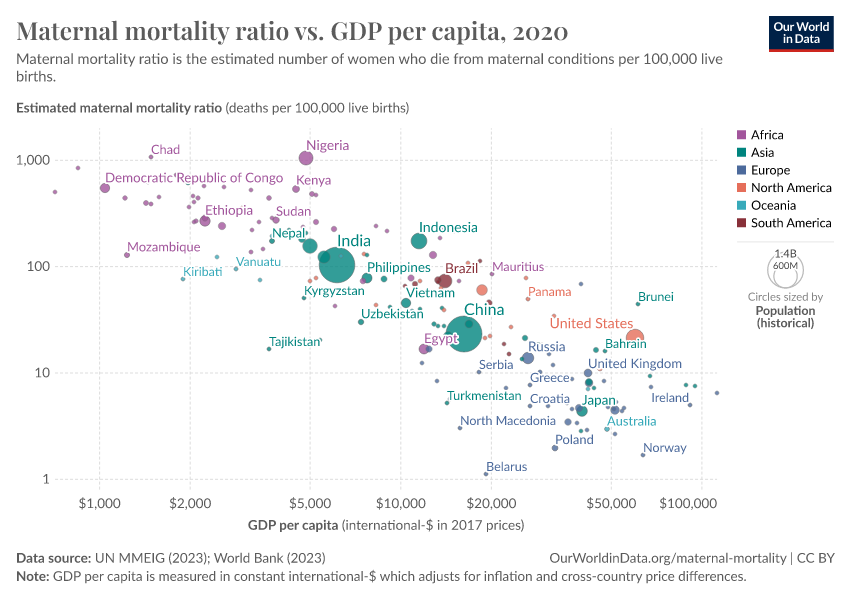
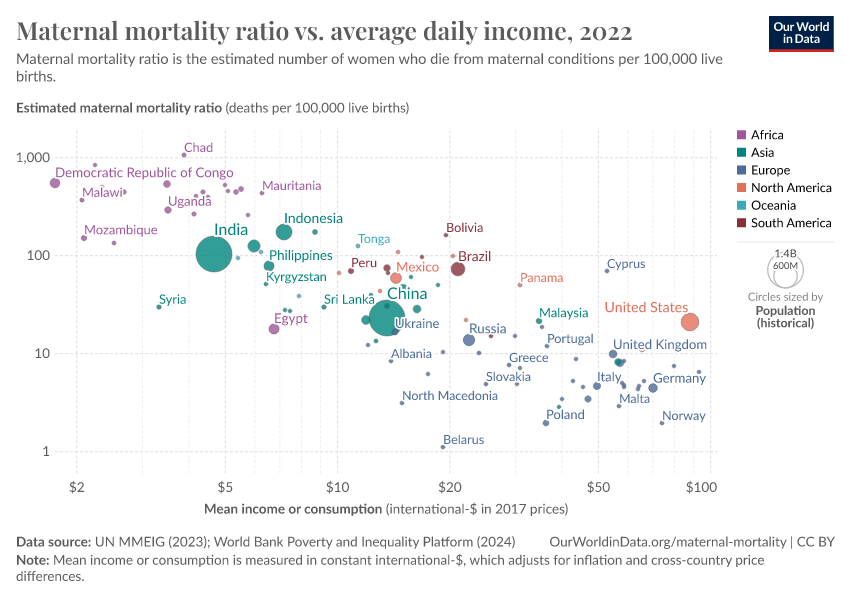
Does maternal mortality fall as countries get richer?
This chart shows the relationship between the maternal mortality ratio and the average income across the world.
There is a strong correlation: the maternal mortality rate is lower in countries with higher incomes.
But not every country that achieved economic growth also reduced maternal mortality. The large spread of countries at a given level of income makes clear that there is more than income that matters here: healthcare and nutrition also play a big role.

Key Charts on Maternal Mortality
See all charts on this topic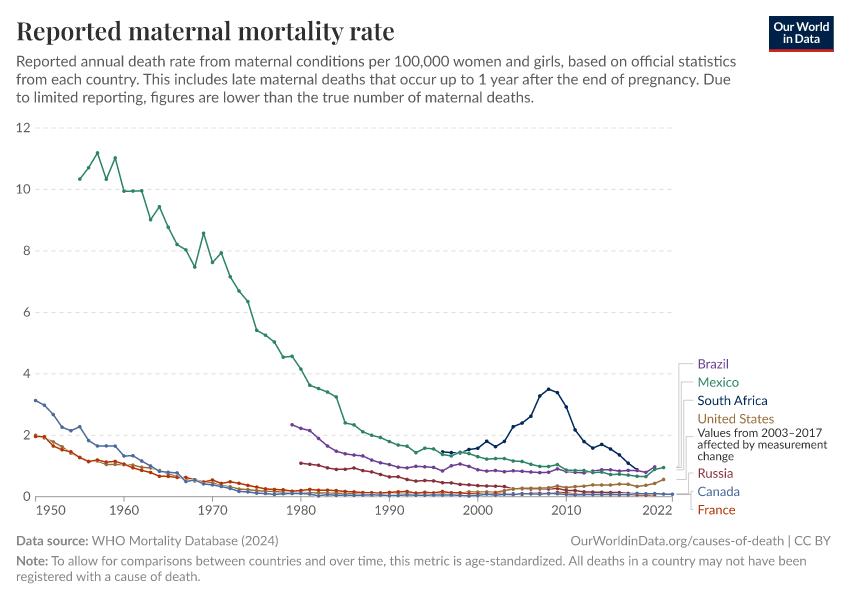
















Featured Data on Maternal Mortality
Endnotes
See Kenneth Hill — Methods for Measuring Maternal Mortality here.
Here we assume a global maternal mortality rate of 900 per 100,000 live births in 2015. The UN estimates there were around 140 million births in 2015. This works out at around 1.26 million pregnancy-related deaths [140 million / [900 / 100,000] = 1.26 million].
Here we assume a global maternal mortality rate of 8 per 100,000 live births in 2015. The UN estimates there were around 140 million births in 2015. This works out at around 11,000 pregnancy-related deaths [140 million / [8 / 100,000] = 11,000].
This of course opens up a much larger question of how many deaths are actually preventable i.e. how low could maternal mortality go. We base our scenario here on the EU-average rate, but we know some countries have an even lower rate: Finland has a rate of 3 per 100,000 live births; and Sweden has a rate of 4. It’s unclear how attainable this is for all countries, or whether this rate could fall even further.
Irvine Loudon (1992) — The transformation of maternal mortality. BMJ 1992; 305:1557 doi: https://doi.org/10.1136/bmj.305.6868.1557 (Published 19 December 1992)
More information on this history, the data from the two clinics in Vienna, and references to earlier precursors of Semmelweis (whose work was unknown to him) can be found in Irvine Loudon (1992) — Death in Childbirth: An International Study of Maternal Care and Maternal Mortality 1800-1950. Published on Oxford Scholarship Online: http://www.oxfordscholarship.com/view/10.1093/acprof:oso/9780198229971.001.0001/acprof-9780198229971 Loudon, I. (2013). Ignaz Phillip Semmelweis' studies of death in childbirth. Journal of the Royal Society of Medicine, 106(11), 461-463. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3807776/
Cite this work
Our articles and data visualizations rely on work from many different people and organizations. When citing this topic page, please also cite the underlying data sources. This topic page can be cited as:
Max Roser and Hannah Ritchie (2013) - “Maternal Mortality” Published online at OurWorldinData.org. Retrieved from: 'https://ourworldindata.org/maternal-mortality' [Online Resource]BibTeX citation
@article{owid-maternal-mortality,
author = {Max Roser and Hannah Ritchie},
title = {Maternal Mortality},
journal = {Our World in Data},
year = {2013},
note = {https://ourworldindata.org/maternal-mortality}
}Reuse this work freely
All visualizations, data, and articles produced by Our World in Data are completely open access under the Creative Commons BY license. You have the permission to use, distribute, and reproduce these in any medium, provided the source and authors are credited.
The data produced by third parties and made available by Our World in Data is subject to the license terms from the original third-party authors. We will always indicate the original source of the data in our documentation, so you should always check the license of any such third-party data before use and redistribution.
All of our charts can be embedded in any site.